🧵 Whatever your views on assisted dying, one thing I’d hoped we’d all agree on is that the topic is ethically fraught & complex.
Not so Matthew Parris.
For him, it’s simple. Old & frail people *should* be killed - to save society the cost of looking after them. 1/n
Not so Matthew Parris.
For him, it’s simple. Old & frail people *should* be killed - to save society the cost of looking after them. 1/n
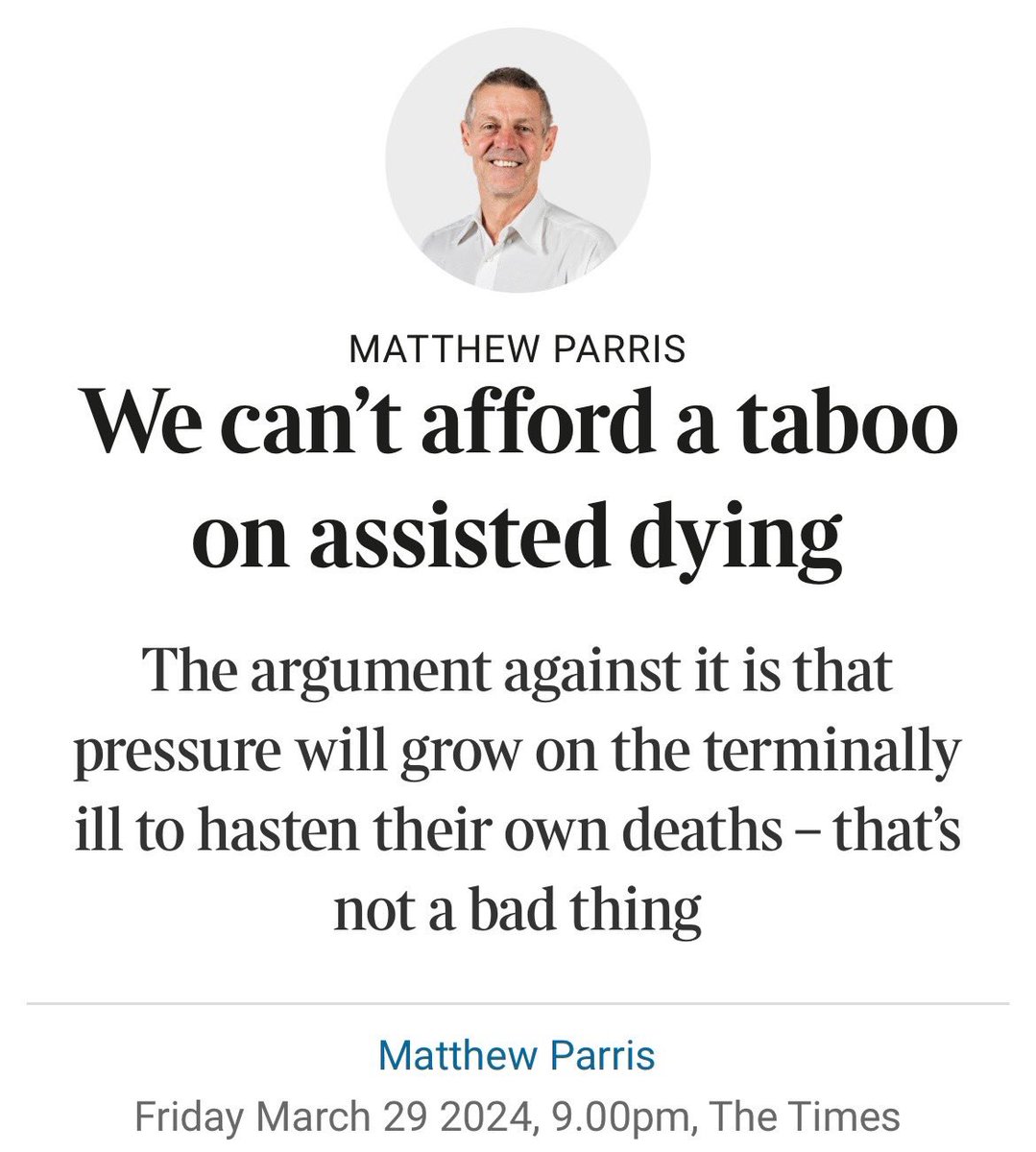
In no sense am I twisting Parris’s words.
Here he rehearses an argument often used by opponents of AD to fight legal change - that with time, it will lead to people feeling pressured to end their lives prematurely (for it would be socially irresponsible of them not to). 2/n
Here he rehearses an argument often used by opponents of AD to fight legal change - that with time, it will lead to people feeling pressured to end their lives prematurely (for it would be socially irresponsible of them not to). 2/n

Parris, you’ll have noted, takes that argument to a chilling extreme. He imagines compulsion/coercion being used - a world in which AD would be “urged upon” people.
And far from rejecting that world, he positively embraces it. 3/n
And far from rejecting that world, he positively embraces it. 3/n

But why - how - could this former MP & current Times columnist possibly welcome a future in which society’s most vulnerable members are, in all seriously, compelled to end their lives prematurely?
Answer: we simply can’t afford to carry their burdensome weight any longer. 4/n
Answer: we simply can’t afford to carry their burdensome weight any longer. 4/n


He’s careful in that last paragraph to contradict his previous words, saying euthanasia will not be an “order” (he’s literally just endorsed it being “urged upon” people).
People whose economic output has waned yet who still insist on sponging off society, sorry, living. 5/n
People whose economic output has waned yet who still insist on sponging off society, sorry, living. 5/n
Parris, in short, is entirely at ease with carving up society into two categories of people - those who deserve to live and those who do not.
The frail, old, disabled, vulnerable (perhaps we could group them together as the herd) are society’s burden, its fiscal drag. 6/n
The frail, old, disabled, vulnerable (perhaps we could group them together as the herd) are society’s burden, its fiscal drag. 6/n
How could they possibly imagine Britain can afford to subsidise their worthless existence?
If they won’t “choose” the decent thing, the painless cull, then economic realities must impose it upon them. 7/n
If they won’t “choose” the decent thing, the painless cull, then economic realities must impose it upon them. 7/n
That fact that we *can* apparently afford to spend £1.8 million per person sending refugees to Rwanda seemingly passes Parris by.
(Or maybe he’d sneak them onto the cull list too, for reasons of economic necessity, you understand.) 8/n
(Or maybe he’d sneak them onto the cull list too, for reasons of economic necessity, you understand.) 8/n

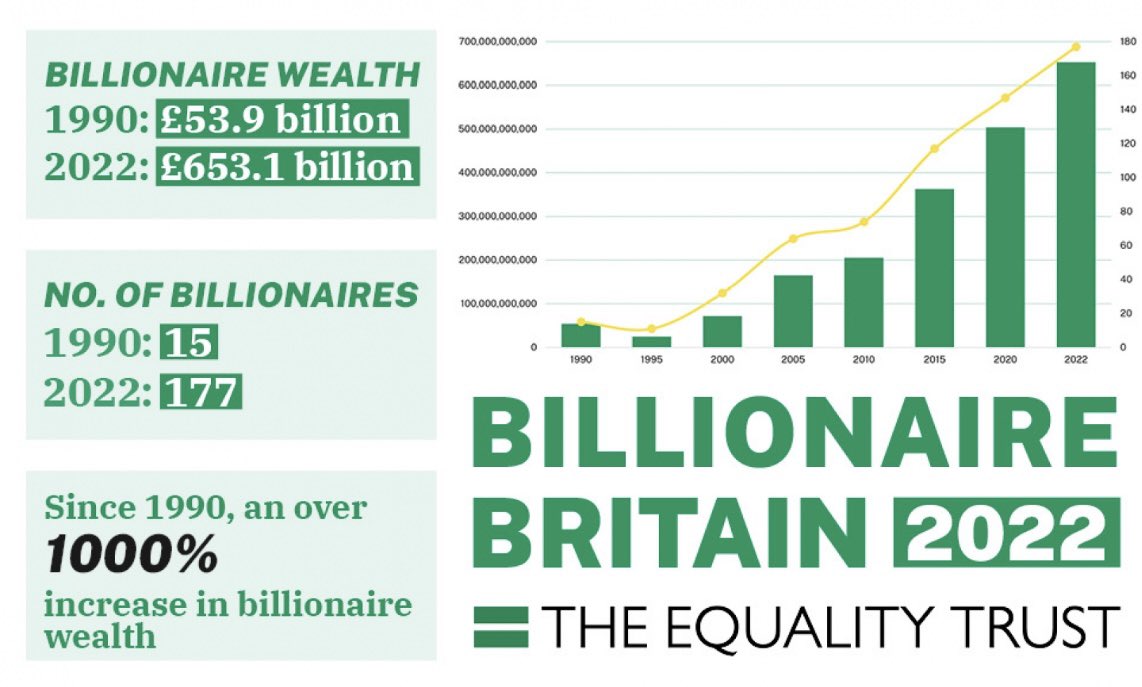
The economics of his argument are obvious nonsense, as demonstrated by the thousandfold increase in billionaire wealth since 1990.
How many frail lives could that £600 billion pounds help support, for example, as opposed to a tiny number of obscenely lavish lifestyles. 10/n
How many frail lives could that £600 billion pounds help support, for example, as opposed to a tiny number of obscenely lavish lifestyles. 10/n
But what horrifies me in this piece is its normalisation of a two tier society in which humanity is carved up into two categories - the deserving (of life) & the purely expendable.
It is one of the most foul things I’ve ever read in a British newspaper. Monstrous, frankly. 11/n
It is one of the most foul things I’ve ever read in a British newspaper. Monstrous, frankly. 11/n
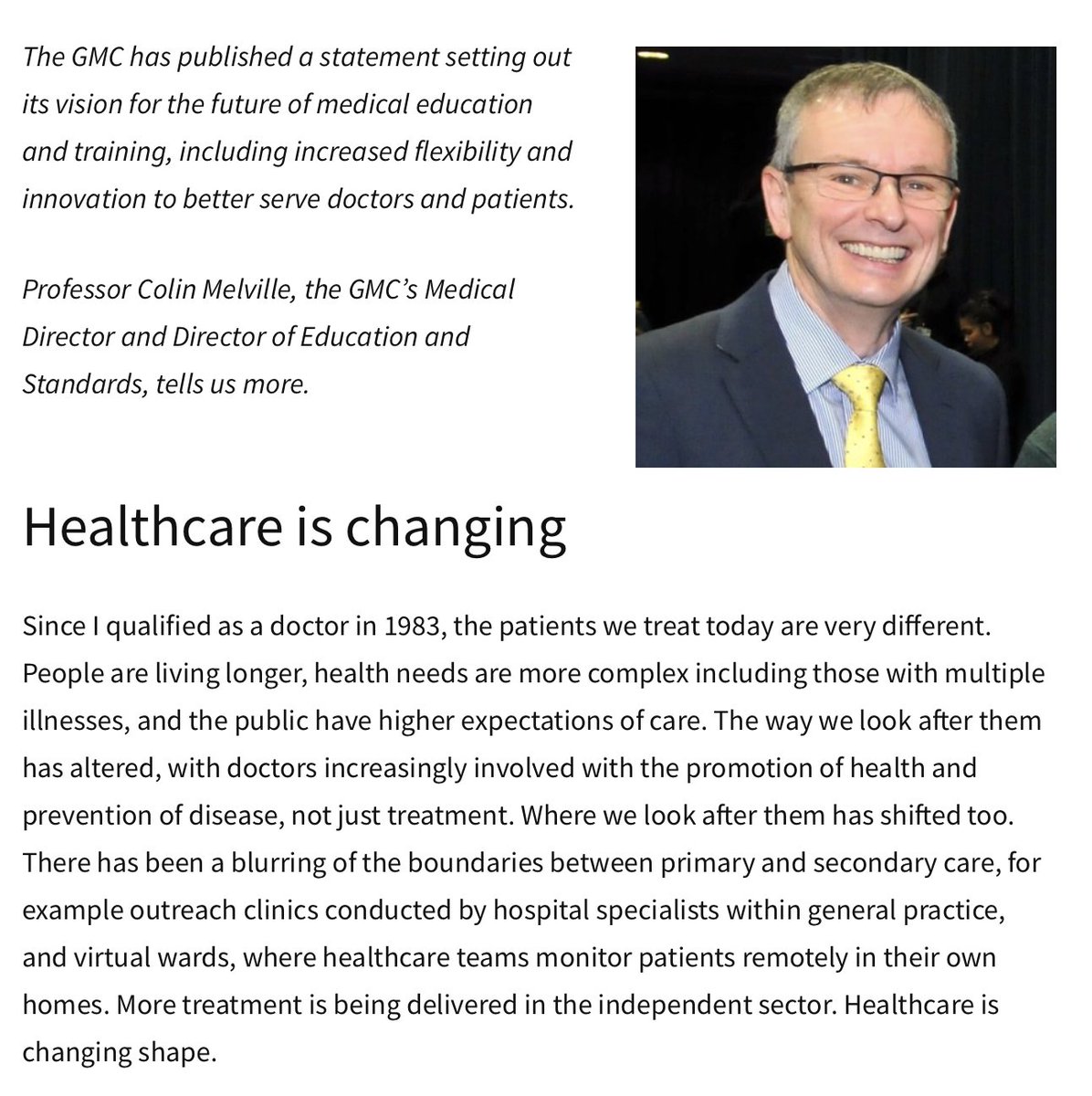
I happen to be deeply biased, of course.
As I palliative care doctor, I work with exceptionally frail, vulnerable, dying patients every day at work.
My bias, if it is that, is grounded in experience.
So let me tell you what I see. 12/n
As I palliative care doctor, I work with exceptionally frail, vulnerable, dying patients every day at work.
My bias, if it is that, is grounded in experience.
So let me tell you what I see. 12/n
I see human beings who are anguished, exhausted, bewildered & afraid - yet whose strength, courage, dignity, compassion, wit, intelligence, generosity, integrity, cheer & grace astound me daily.
I see the best of humanity. Of us. Our species.
Every single day at work. 13/n
I see the best of humanity. Of us. Our species.
Every single day at work. 13/n
And the notion that my patients - who one day, without fail, will be you, me, all of us - do not deserve to live because they can’t do paid work is absolutely sickening. 14/n
There are many powerful arguments in favour of AD, but this piece by Matthew Parris couldn’t be more compelling as an argument against.
And that he put it out there, in the mainstream, with not a shred of shame.
The worthy - and the herd to be culled.
I’m sickened. Ends/
And that he put it out there, in the mainstream, with not a shred of shame.
The worthy - and the herd to be culled.
I’m sickened. Ends/
Postscript. Long ago I made a deliberate choice not to state my personal views on AD in public - out of concern that this could potentially jeopardise my relationship with my patients. That still stands.
However, the prospect of AD putting pressure on vulnerable people to end their lives prematurely is clearly worrying, particularly given the evidence of this occurring in countries such as Canada, where AD is legal.
But not once did I imagine the view entering the mainstream that - far from protecting elderly, disabled & vulnerable people with strict safeguards around AD - we should pro-actively push them into premature death on grounds of economic expediency. Matthew Parris's views are grotesque.
However, the prospect of AD putting pressure on vulnerable people to end their lives prematurely is clearly worrying, particularly given the evidence of this occurring in countries such as Canada, where AD is legal.
But not once did I imagine the view entering the mainstream that - far from protecting elderly, disabled & vulnerable people with strict safeguards around AD - we should pro-actively push them into premature death on grounds of economic expediency. Matthew Parris's views are grotesque.
• • •
Missing some Tweet in this thread? You can try to
force a refresh