
The final report of the Cass Review is out
England's National Health Service commissioned this independent review, by pediatrician Hilary Cass, of the nation's just-closed pediatric gender care clinic and the research backing pediatric gender-transition treatment.
Learn more🧵⬇️
England's National Health Service commissioned this independent review, by pediatrician Hilary Cass, of the nation's just-closed pediatric gender care clinic and the research backing pediatric gender-transition treatment.
Learn more🧵⬇️

The Cass Review characterizes the medicalized approach to pediatric gender-transition treatment—one that all major US medical societies support, and which is centered around the prescription of puberty blockers and cross-sex hormones—as unsupported by sound scientific evidence.🧵
“There remains diversity of opinion as to how best to treat these...young people. The evidence is weak and clinicians have told us they are unable to determine with any certainty which children and young people will go on to have an enduring trans identity.” –The Cass Review

While the Cass Review is measured in tone, it nevertheless offers a scathing critique England’s erstwhile pediatric gender clinic's efforts to care for the fast expanding population of adolescents, in particular biological girls, burdened by severe gender-related distress.

The Cass Review was published in concert with a raft of peer-reviewed analyses of the evidence base and global treatment guidelines regarding pediatric gender medicine. Cass commissioned those studies from researchers at York University.
adc.bmj.com/pages/gender-i…
adc.bmj.com/pages/gender-i…

Like previous systematic literature reviews, the York University reviews found the evidence backing pediatric gender-transition treatment wanting and largely of low quality. adc.bmj.com/pages/gender-i…
The Cass Review reports that research does *not* support the claim that puberty blockers and hormones reduce the elevated suicide death rate among gender-distressed youths. Thus the claim that pediatric gender-transition treatment is “life saving" is not evidence based.

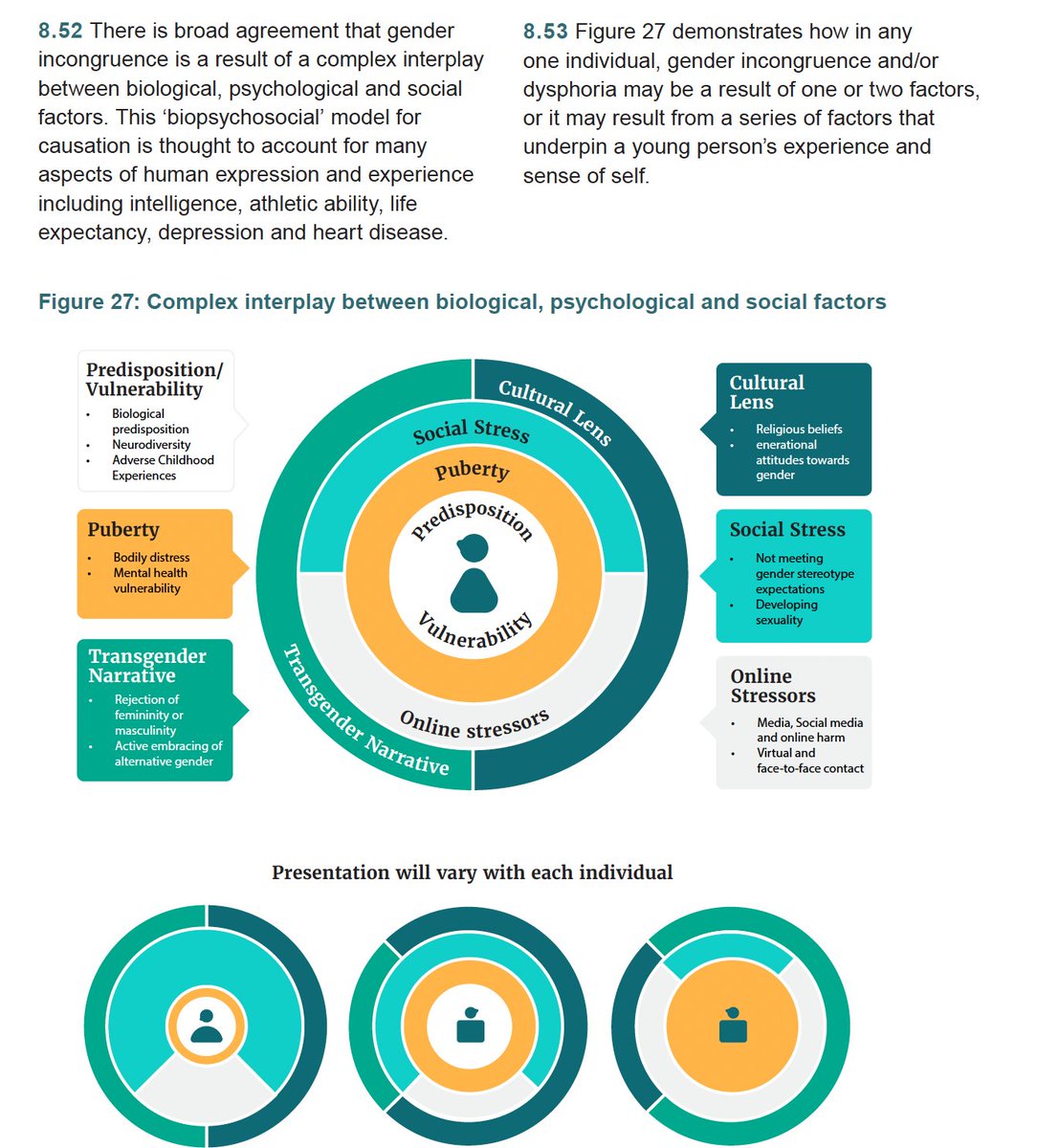
“There is no simple explanation for the increase in the numbers of predominantly young people" identifying as transgender, "but there is broad agreement that it is a result of a complex interplay between biological, psychological and social factors." --The Cass Review
The Cass review acknowledges the NHS's recent decision to permit hormones for gender distressed youths starting at age 16. But Cass advises "extreme caution" and a "clear clinical rationale" for starting before age 18.

Cass advises that families considering social transitioning gender-incongruent children—changing a child’s name, pronouns, clothing, etc.—should take into account that this “may change the trajectory of gender identity development.”

The systematic literature review on puberty blockers found: “No conclusions can be drawn about the impact on gender dysphoria, mental and psychosocial health or cognitive development. Bone health and height may be compromised during treatment.” adc.bmj.com/pages/gender-i…

The systematic literature review on hormones for adolescents found: “Moderate-quality evidence suggests mental health may be improved during treatment, but robust study is still required. For other outcomes, no conclusions can be drawn.” adc.bmj.com/pages/gender-i…

The Cass report undermines the primary explicit purpose for puberty blockers, the argument waged by WPATH, American medical associations and others: that they afford children and their families more time to determine whether taking cross-sex hormones is the best option for them.

The Cass report is not simply grounded in systematic literature reviews. It is also based on the team’s years of routine interviews, meetings and focus groups with service providers, families and young people with gender distress, including people who have detransitioned.

“There are few other areas of healthcare where professionals are so afraid to openly discuss their views, where people are vilified on social media, and where name-calling echoes the worst bullying behaviour. This must stop.”
–Dr. Hilary Cass, the Cass Review
–Dr. Hilary Cass, the Cass Review

“Some practitioners abandoned normal clinical approaches to holistic assessment, which has meant that this group of young people have been exceptionalised compared to other young people with similarly complex presentations."
–Dr. Hilary Cass, the Cass Review
–Dr. Hilary Cass, the Cass Review
The Cass Review expressed dismay that England's pediatric gender clinic, GIDS, refused to share its data on the approximately 9,000 children that the clinic has seen since it began prescribing puberty blockers in 2011. This has thwarted Cass's efforts to improve services.

“Young people’s sense of identity is not always fixed and may evolve over time,” the Cass Review states. Whilst some young people may feel an urgency to transition, young adults looking back at their younger selves would often advise slowing down.”
The Cass Review, it states “is cognisant of the broader cultural and societal debates relating to the rights of transgender people. It is not the role of the Review to take any position on the beliefs that underpin these debates.”

To download a copy of the Cass Review's final report, try this link: wetransfer.com/downloads/f1ff…
Most pediatric gender transition treatment guidelines, the Cass Review states, acknowledge the “insufficient evidence about the risks and benefits” of such treatment. Nevertheless, “many then went on to cite this same evidence to recommend medical treatments.”

Cass faulted WPATH and the Endocrine Society for “circularity” in their citations to one another. WPATH “cited many of the other national & regional guidelines to support some of its recommendations." But these guidelines were “considerably influenced” by WPATH’s own guidelines.

While acknowledging that the evidence base behind psychological interventions for youth gender distress are weak, the Cass Review defends against accusations that anything less than a fully “affirmative” approach is tantamount to conversion therapy.

The recommendation from the Cass Review that “long-standing gender incongruence should be an essential prerequisite for medical treatment” suggests that the NHS puberty blocker clinical trial will exclude those with adolescent onset gender dysphoria.

The Cass Review speaks scornfully about the NHS’s recent decision to permit 16 and 17 year olds to access cross-sex hormones.

The new NHS youth gender clinics, the Cass Review states, "should include psychiatrists, paediatricians, psychologists, psychotherapists, clinical nurse specialists, social workers, specialists in autism..., speech and language therapists, occupational health specialists."
“This Review is not about defining what it means to be trans, nor is it about undermining the validity of trans identities, challenging the right of people to express themselves, or rolling back on people’s rights to healthcare,” writes Dr. Hilary Cass.
“We have to start from the understanding that this group of children and young people are just that; children and young people first and foremost, not individuals solely defined by their gender incongruence or gender-related distress.” –Dr. Hilary Cass

“We have to start from the understanding that this group of children and young people are just that; children and young people first and foremost, not individuals solely defined by their gender incongruence or gender-related distress.”
–Dr. Hilary Cass, the Cass Review
–Dr. Hilary Cass, the Cass Review

The Cass Review, it states “is cognisant of the broader cultural and societal debates relating to the rights of transgender people. It is not the role of the Review to take any position on the beliefs that underpin these debates.”

The Cass Review does not come down on any one side of the debate over whether trans identity is inborn, subject to a social-contagion effect, or is the result of any other particular factors. Instead, it suggests an "all of the above" and "it depends" framework.
On the very controversial subject of at what rate pre-pubescent children with early gender incongruence or distress will see this resolve and identify as their birth sex by adolescence, known as desisting, the Cass Review says that the desistance rate is apparently high.

The Cass Review expressed concerns that many of the same factors that have made caring for gender distressed children and adolescents so fraught and complex will likely remain true for young adults. So it recommends the NHS look at the service for that demographic as well.

The Cass Review insists that the needs of detransitioners--those who have medically transitioned to the opposite sex and who have reverted to identifying and presenting as their biological sex--must not be overlooked.

The Cass Review expressed concerns about young people turning to unregulated clinics to obtain puberty blockers now that the NHS has ceased prescribing them.
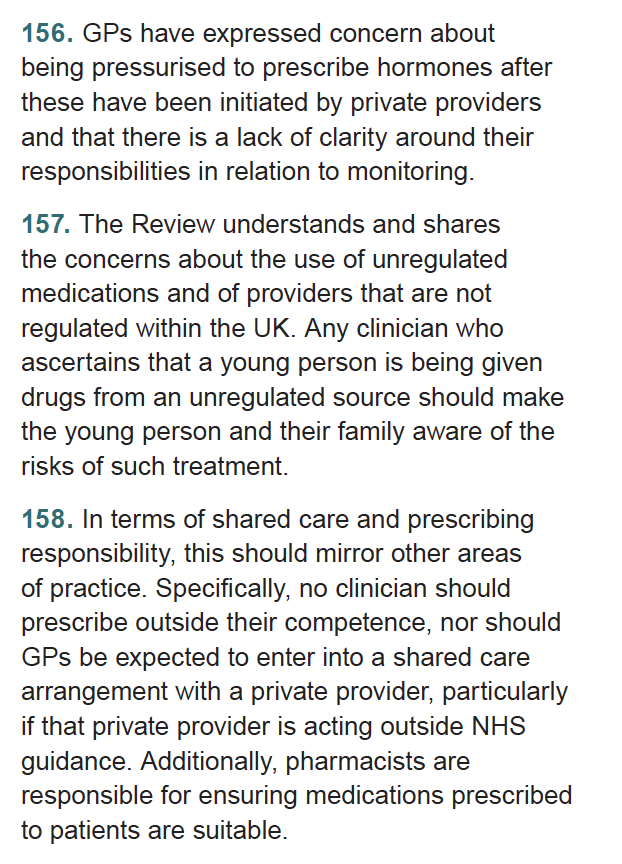
The Cass Review recommended clamping down on pharmacists' doling out puberty blockers now that the NHS has ceased newly prescribing them. (Minors currently on the drugs will be allowed to stay on them.)

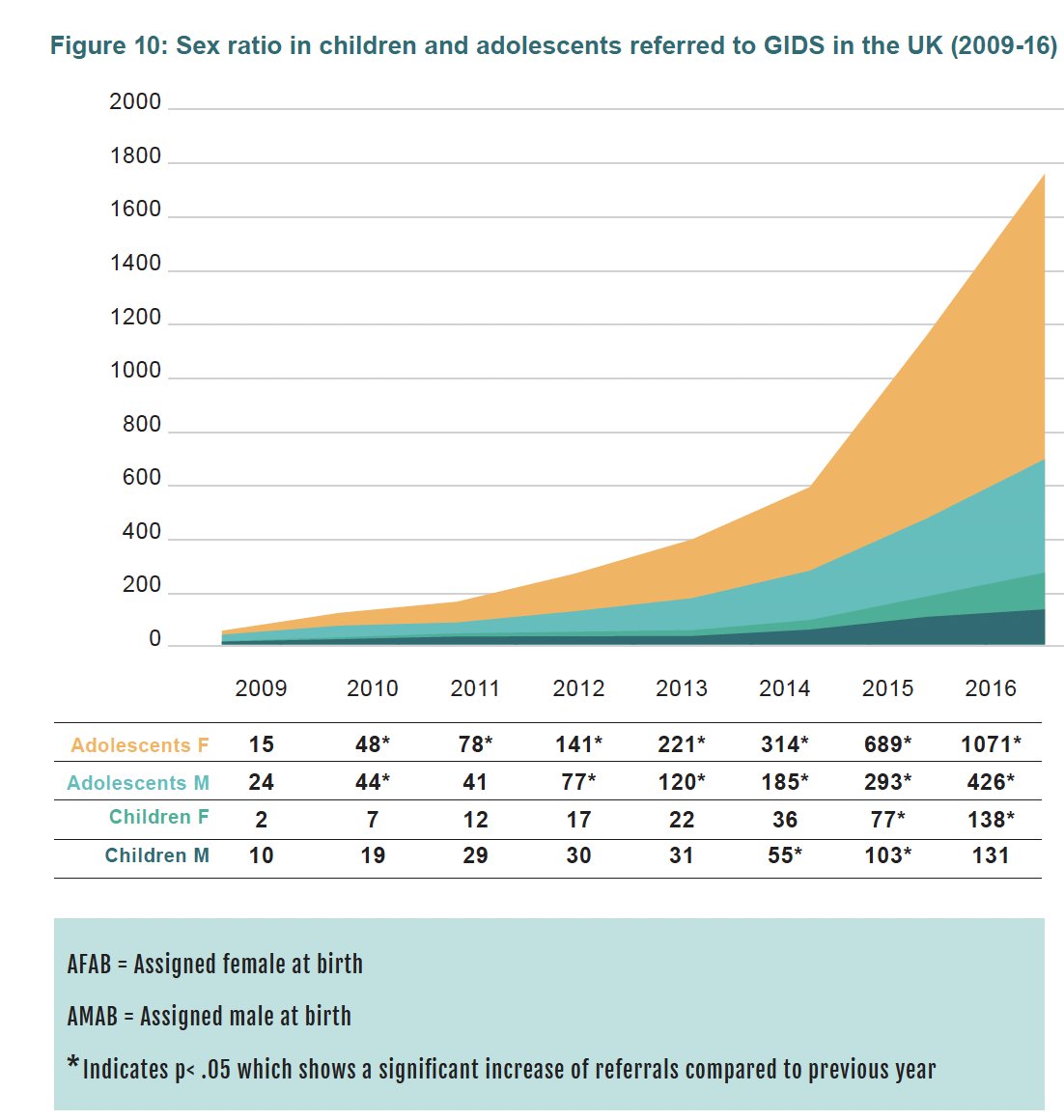
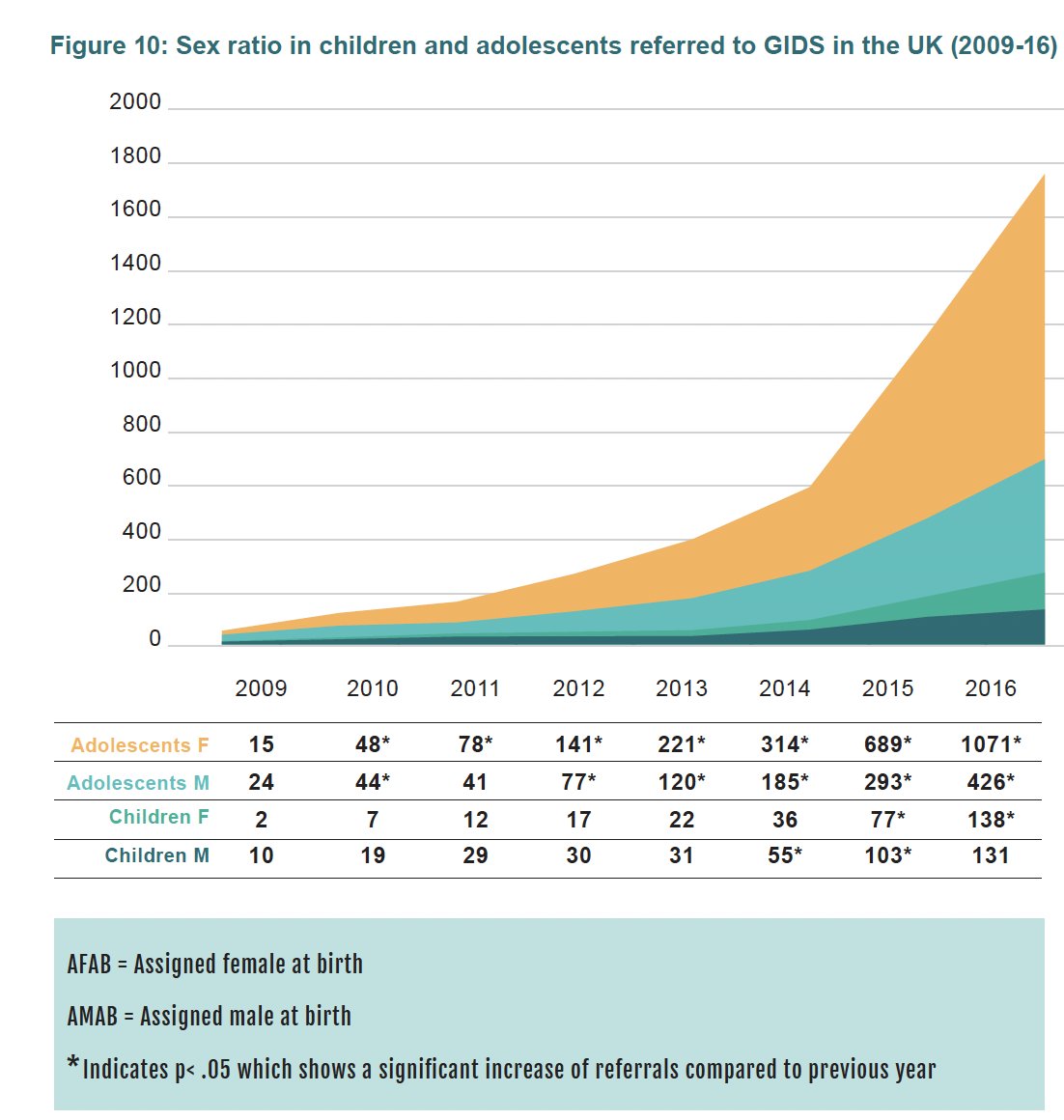
This chart of the children and adolescents referred to the NHS's now-shuttered pediatric gender clinic, GIDS, demonstrates a common worldwide phenomenon: a surge of gender dysphoria and trans identification in about 2014, especially among biological girls.
This extended chart shows the continued surge in referrals to the NHS's pediatric gender clinic, GIDS, through 2021 to 2022, largely among older biological girls. (In the most recent years, they stopped reporting biological sex.)
The Cass Review had the following to say about the study published in February about the risk of suicide death among youths referred to gender clinics in Finland (which I covered for @NYPost-- ): nypost.com/2024/02/24/opi…

The Cass Review said that the dramatic change in the patient profile in those presenting with pediatric gender distress in England needs to be reflected by the services NHS offers.

The striking increase" in youth gender distress "needs to be considered within the context of poor mental health and emotional distress amongst the broader adolescent population, particularly given their high rates of co-existing mental health problems and neurodiversity."

The Cass Review suggests a connection between the youth mental health crisis overall and the influx of young people developing gender-related distress.

Nodding to the recent book by @JonHaidt, The Anxious Generation, the Cass Review points to a sudden rise in self harm in 13 to 16 year old girls in the early 2010s. This preceded the spike among biological girls identifying as trans.

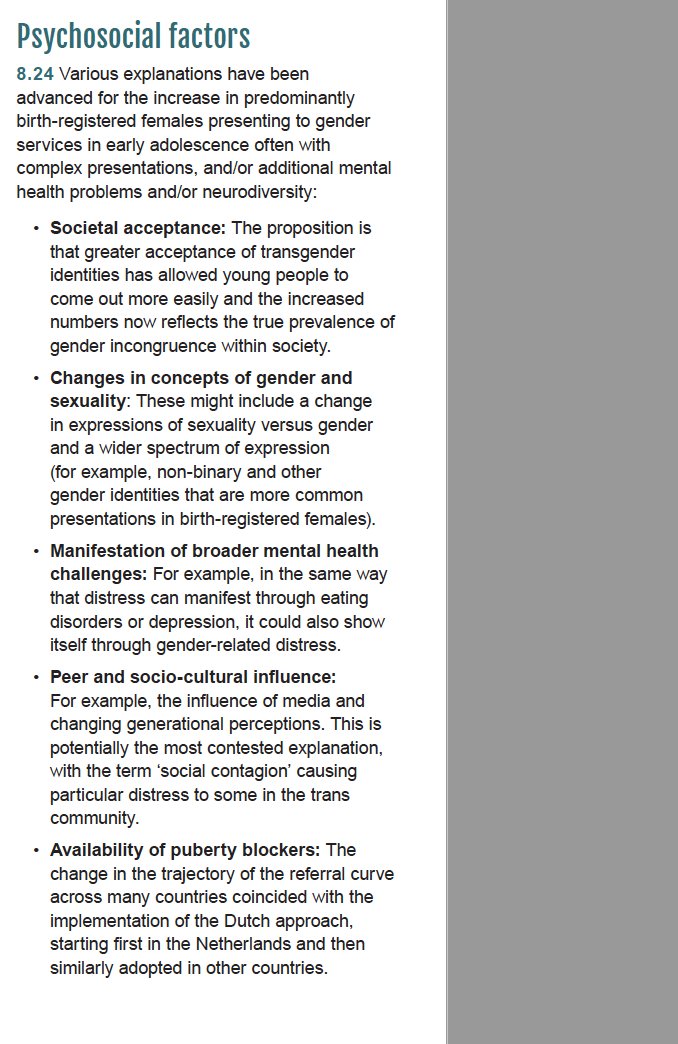
The Cass Review ticks off various psychosocial factors that may drive trans identification in youth.
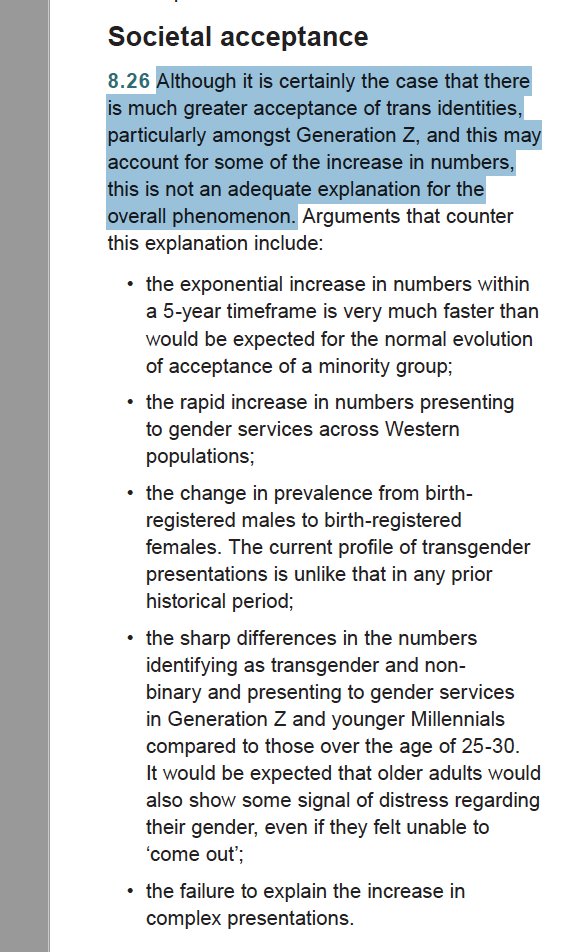
It is common to hear the argument that wide social acceptance is the sole reason for the recent rise in trans identification in youths. Activists often point to the supposed rise in left handedness after that stopped being scorned as a parallel. The Cass Review isn't convinced.
The new systematic literature review of the more than 20 pediatric gender care guidelines led the Cass Review to conclude that it could only recommend the Finnish and Swedish guidelines. WPATH and American Academy of Pediatrics got notably low scores.

The Cass Report says "it is important to view" social transitioning--changing name, pronouns, dress, hair, etc.--"as an active intervention because it may have significant effects on the child or young person in terms of their psychological functioning or longer-term outcomes."

The Cass Review reports that when gender-distressed children socially transition and keep their biological sex secret at school, this may drive them to want to go on puberty blockers to avoid "being found out".

Of the 11 available studies on social transition, nine were low quality, including @Jack_Turban 2022 and Olson 2016 and 2022; and two were moderate quality, including Steensma 2013 and Sievert 2021.

WPATH recently shifted from a cautious to an enthusiastic support for socially transitioning children. "However," the Cass Review states, "none of the WPATH 8 statements in favor of social transition in childhood are supported by the findings of the" systematic literature review.

The Cass Review differed sharply with WPATH, advising a "cautious approach" to socially transitioning children with gender incongruence or distress.

Cass Review finishes: "While open and constructive debate is needed, I would urge everybody to remember the children & young people trying to live their lives and the families/carers and clinicians doing their best to support them. All should be treated with compassion & respect.

@threadreaderapp unroll

Here is a working link for the multiple systematic literature reviews on which the English Cass Review of pediatric gender medicine was based. adc.bmj.com/content/early/…

• • •
Missing some Tweet in this thread? You can try to
force a refresh
















