
On Sat, @SpinalCSFCanada put on the 1st spinal CSF leak conference in Canada. Below, some screenshots of slides & thoughts on some of the talks. 🧵
(For those new to leaks: SIH = spontaneous intracranial hypotension. The conf did have talks for non-spontaneous leaks though!)
(For those new to leaks: SIH = spontaneous intracranial hypotension. The conf did have talks for non-spontaneous leaks though!)
Personal background: my spinal CSF leak was due to a 2017 bedside lumbar puncture in the ER. I have been leaking since 2017 & repairs have not held. Shared my story for CNN Travel in 2022:
Disclosure: I'm on the Board of the US @spinalCSFleak nonprofit. cnn.com/travel/article…
Disclosure: I'm on the Board of the US @spinalCSFleak nonprofit. cnn.com/travel/article…

Ok diving in to some of the slides!
1/ A summary of the decision tree for different leak fact patterns, as presented by Dr. Linda Gray of @DukeRadiology, who started their spinal CSF leak program.
See my next tweet for ventral leaks, which she also discussed in her talk.
1/ A summary of the decision tree for different leak fact patterns, as presented by Dr. Linda Gray of @DukeRadiology, who started their spinal CSF leak program.
See my next tweet for ventral leaks, which she also discussed in her talk.

In this slide, a LP patient got a patch targeted at a ventral leak (a leak at the front of the body).
Duke pioneered this technique ().
As my leak is suspected to be ventral, I received this kind of patching. It's called a transforaminal approach. pubmed.ncbi.nlm.nih.gov/27390315/
Duke pioneered this technique ().
As my leak is suspected to be ventral, I received this kind of patching. It's called a transforaminal approach. pubmed.ncbi.nlm.nih.gov/27390315/

I hope more & more Drs offer this patch/technique as a next step for post-puncture patients when dorsal patching fails. If I hadn't gone to a specialty centre, I wouldn't have had the opportunity. I hear from patients where dorsal EBPs fail & they're just told 'nope, no leak' 💔
2) Stanford's Dr. Ian Carroll, who presented about the problem of "Persistent Post-Puncture Headache" — hi, it's me!
This can be referred to as cPDPH (chronic post-puncture headache) or pPDPH (persistent PDPH).
Here's what it looks like in surgery: an unhealed hole.
This can be referred to as cPDPH (chronic post-puncture headache) or pPDPH (persistent PDPH).
Here's what it looks like in surgery: an unhealed hole.

A 2024 study about pPDPH found that it can last for years, challenging the ICHD-3 classification that says it 'remits spontaneously w/in 2 weeks'. Low quality of life scores, depression, disability, etc occur with the condition: …alofheadacheandpain.biomedcentral.com/articles/10.11…
A large factor for spinal CSF leak after a puncture = the type of needle tip.
Per the data as presented by Dr. Carroll, cutting or traumatic needles (e.g. Quincke type) should be avoided in favour of an atraumatic needle tip (e.g. Whitacre, Gertie-Marx, etc.)
Per the data as presented by Dr. Carroll, cutting or traumatic needles (e.g. Quincke type) should be avoided in favour of an atraumatic needle tip (e.g. Whitacre, Gertie-Marx, etc.)

He shared a few studies to that end, incl. "Atraumatic (pencil-point) versus conventional needles for lumbar puncture":
The right slide shows the results that atraumatic needles are favoured for almost all benefit & harm outcomes. bmj.com/content/361/bm…
The right slide shows the results that atraumatic needles are favoured for almost all benefit & harm outcomes. bmj.com/content/361/bm…


In a different study, comparing the needle tips, the authors found no increased failure rate when using an atraumatic needle, but DID find a decrease in PDPH, concluding atraumatic needles are "a superior option for patients who require lumbar puncture." thelancet.com/journals/lance…

Slide illustrating the difference in shape & rates of post puncture dural headache (PDPH*):
*Eventually, I hope PDPH is changed to 'post puncture spinal CSF leak'. The awful occipital pain when your brain sinks due to a leak doesn't feel like a headache to me, or to many others.
*Eventually, I hope PDPH is changed to 'post puncture spinal CSF leak'. The awful occipital pain when your brain sinks due to a leak doesn't feel like a headache to me, or to many others.

Dr. Carroll noted it's impt for physicians to ask chronic spinal CSF leak patients about prior dural puncture (epidural/LP). Eg, in this 2023 study where a bleb—a type of arachnoid herniation that can occur during a puncture—was symptomatic years later. …adachejournal.onlinelibrary.wiley.com/doi/full/10.11…
He ended w/ a firm CTA for physicians to switch to atraumatic needles despite being a bit more $, & a QR code for access to resources.
Some Drs who read LN wrote in to say their hospitals said no to atraumatic needles due to cost, despite better outcomes. Hope that changes.
Some Drs who read LN wrote in to say their hospitals said no to atraumatic needles due to cost, despite better outcomes. Hope that changes.

Moving on! 3) Dr @WouterSchievink's talk about SIH stressed that a "CSF leak centre" referral is less crucial in early stages than access to timely EBPs, even if a CSF leak hasn't yet been localized. (Because patients may be pinged around and/or denied an EBP w/out a leak site.)
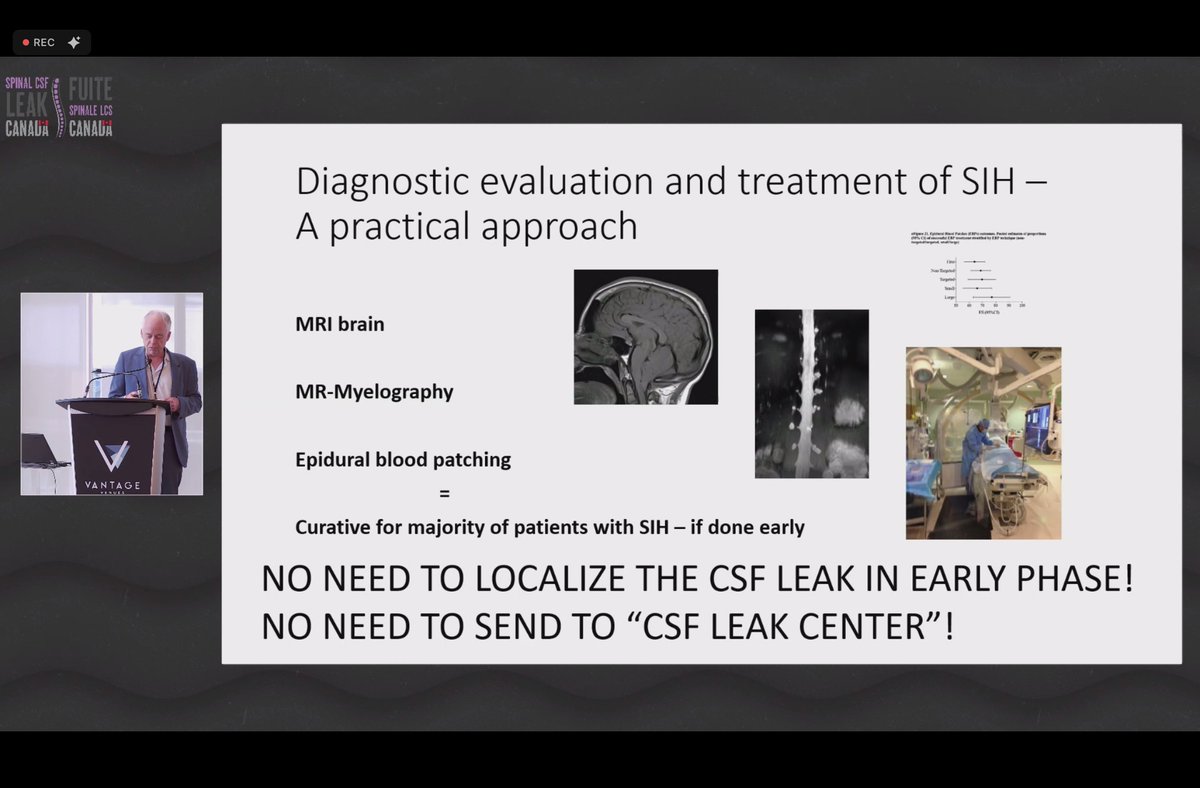
@WouterSchievink I'm 👀 on any ventral spinal CSF leak imaging. Look at the size of that tear on the right, wowza. These tears are different to the puncture hole shared upthread; Dr. Schievink's talk was primarily about SIH. Causes for a tear like this can include calcified disks & osteophytes.

@WouterSchievink Moving on to 4) Dr. Ulrich, a neurosurgeon in Bern, Switzerland. Two slides below a) on quality of life with cPDPH, & b) the diagnostic workups for those patients — noting it is rare to find a direct leak site for them, even with a CSF leak protocol used for the MRI machine:

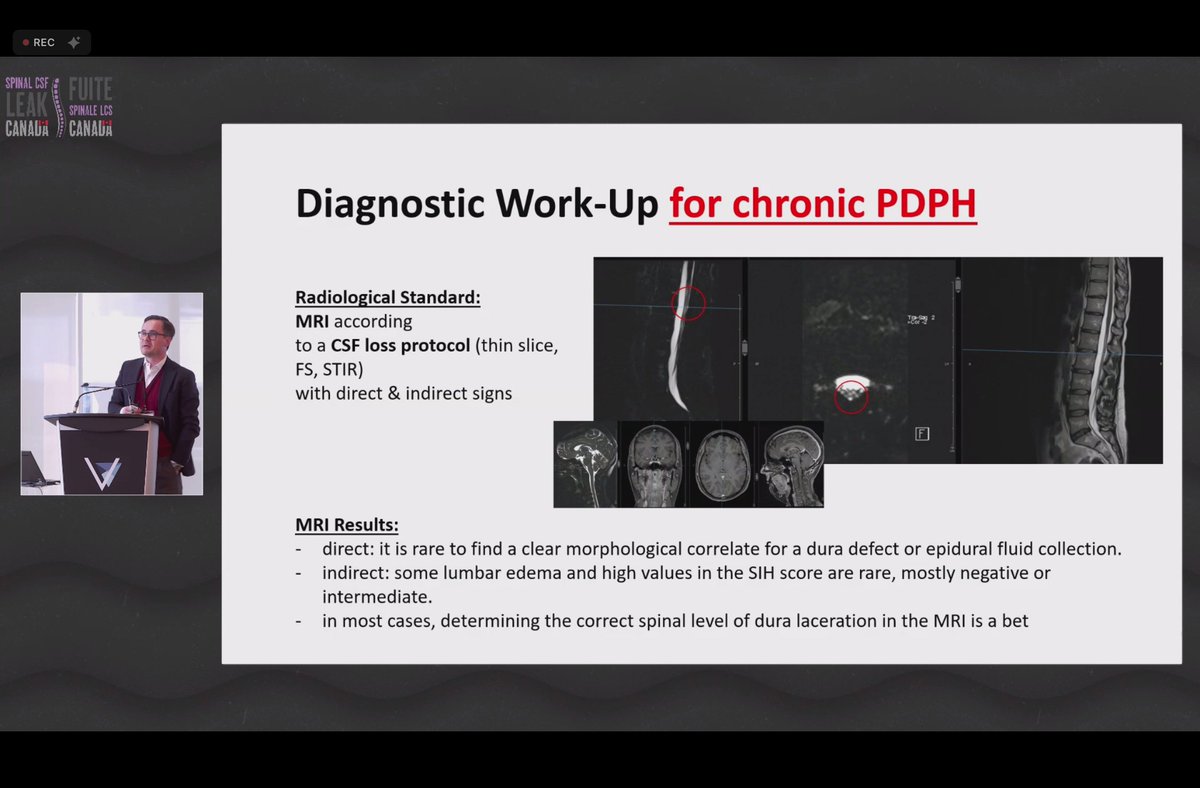
@WouterSchievink I appreciated that he discussed non-successes, cases like mine where repairs haven't held (tho I haven't yet had surgery, just fibrin/glue patching). Case below of a previously healthy woman; imaging was neg., repair failed, & revision also failed, w/ only modest improvement.

@WouterSchievink He also shared different types of dural defects found in cPDPH:
-arachnoid blebs—noted earlier;
-ventral dural leaks—👀
-basic defects—'just' a hole
-neomembrane—thin scar tissue covers the hole, but it's not sealed. Needs to be peeled back, then stitch/cover the leak.
-arachnoid blebs—noted earlier;
-ventral dural leaks—👀
-basic defects—'just' a hole
-neomembrane—thin scar tissue covers the hole, but it's not sealed. Needs to be peeled back, then stitch/cover the leak.

@WouterSchievink He also noted that patients may have leaks on multiple levels, and concluded that pPDPH is an underrecognized but severe and debilitating condition where imaging is mostly negative and long term follow up care is needed.


@WouterSchievink 4) Dr. @PeterGKranz talked about RIH, rebound intracranial hypertension. For non leak patients, this is the 'oppositeland' that can occur after a leak is sealed as the body attempts to normalize CSF volume & pressure after compensating for a leak.
Medications to treat it:
Medications to treat it:

@WouterSchievink @PeterGKranz For patients with side effects to CAI med Diamox (acetazolamide), methazolamide may be used. I couldn't tolerate Diamox when sealed, & I took methazolamide instead. Dr @PeterGKranz noted that it has depleted potassium in his patients more than Diamox does/did.

@WouterSchievink @PeterGKranz For more unmanageable RIH, where meds don't suffice, he shared options for acute & chronic treatments. He noted that a shunt is a last resort, and also made note of interesting studies about using GLP-1 meds (what can't they do?!) to treat RIH, e.g.: ahmjournal.com/glucagon-like-…

@WouterSchievink @PeterGKranz Conclusion: rebound intracranial hypertension is NOT rare (though many patients are told it is by non-experts), and needs to be planned for if a doctor is treating spinal CSF leak.

Taking a break but back in a bit for a few more talks / slides!
We're back! Ok, next up 6) was another talk by @WouterSchievink, where he discussed complications of chronic spontaneous spinal CSF leak. Among them, the list below. The image to the right is of a subdural hematoma, a collection of blood that forms on the surface of the brain.

He also discussed how adhesive arachnoiditis could be caused by blood entering the thecal sac due to a CSF venous fistula, causing chronic inflammation that can then lead to a build up of scar tissue. I'd never heard of it in that context, only w/ surgery, LPs, patching, etc.

Adhesive arachnoiditis is a progressive condition that historically is known to be a potential complication of surgeries, EBPs (esp if accidentially punctured during it), LPs, epidurals, CT-myelograms, & more. To hear a non-iatrogenic cause is interesting. It's very painful.
There's tension btwn specialties: if you have AA, AA practitioners caution against procedures—but spinal CSF leak healing often requires them. My imaging showed early stages, & I had associated sx; it's part of why I've been more conservative with repairs. medcentral.com/pain/spine/low…
Next up, 7) Dr. Rosann Seviour talked about challenges to getting diagnosed with SIH here in Canada, including the lack of Canadian data (soon to change!), & that it's rarely taught in med schools or at a 2023 conf. Dr. Seviour attended—attendees only knew of post-LP leaks.

Challenges in diagnosing SIH include: a lack of confirmatory test, MRI being normal for 20% of SIH patients, that ICD classification requirements include <6 opening pressure — but we know now that opening pressure being normal doesn't rule out a spinal CSF leak!

For treatment, in Canada challenges include: no Canadian referral centre (yet!), lack of early tx, no local SIH guidelines (2023 guidelines from UK here: ), & that 1 blood patch isn't curative for many. She estimates a 64% success rate for the first patch. jnnp.bmj.com/content/94/10/…

8) Dr. @YHoydonckx spoke about the results of national survey on SIH care in Canada spearheaded by @SpinalCSFCanada. She noted serious impacts on employment & health, & shared the % of patients who sought treatment at US leak centers, revealing lack of access to care in Canada.


@YHoydonckx @SpinalCSFCanada The survey found that "re-leaking" is common—44% of respondents relapsed after initial treatment.
She concluded by summarizing the findings from this 1st national survey. Great to see data from Canada, as depressing as the findings are—but now we know what to try & change.
She concluded by summarizing the findings from this 1st national survey. Great to see data from Canada, as depressing as the findings are—but now we know what to try & change.


@YHoydonckx @SpinalCSFCanada Next up, 9) Dr. Amoozegar on establishing a SIH registry in Canada, as well as quarterly virtual 'case rounds' for complex SIH cases. I wish this included LP leaks / post-surgical leaks not only SIH, but it's good to see this progress regardless!


@YHoydonckx @SpinalCSFCanada And finally, @SpinalCSFCanada's Bahareh concluded with a moving talk about her own leak journey, and the progress in education and grants from the organization.
This summary was only some of the talks; the full list of presentations is here:
/END spinalcsfleakcanada.ca/program-canadi…
This summary was only some of the talks; the full list of presentations is here:
/END spinalcsfleakcanada.ca/program-canadi…

@YHoydonckx @SpinalCSFCanada @FPDESIGNTO @threadreaderapp unroll please!
• • •
Missing some Tweet in this thread? You can try to
force a refresh



