More Paxlovid clarification. We have:
*clinical trials* showing it:
-reduces the risk of death & hospitalization for those at risk
-did not have benefit in a group of patients with LC
Some *observational studies* showing an association with lower LC risk if taken for acute C19🧵
*clinical trials* showing it:
-reduces the risk of death & hospitalization for those at risk
-did not have benefit in a group of patients with LC
Some *observational studies* showing an association with lower LC risk if taken for acute C19🧵
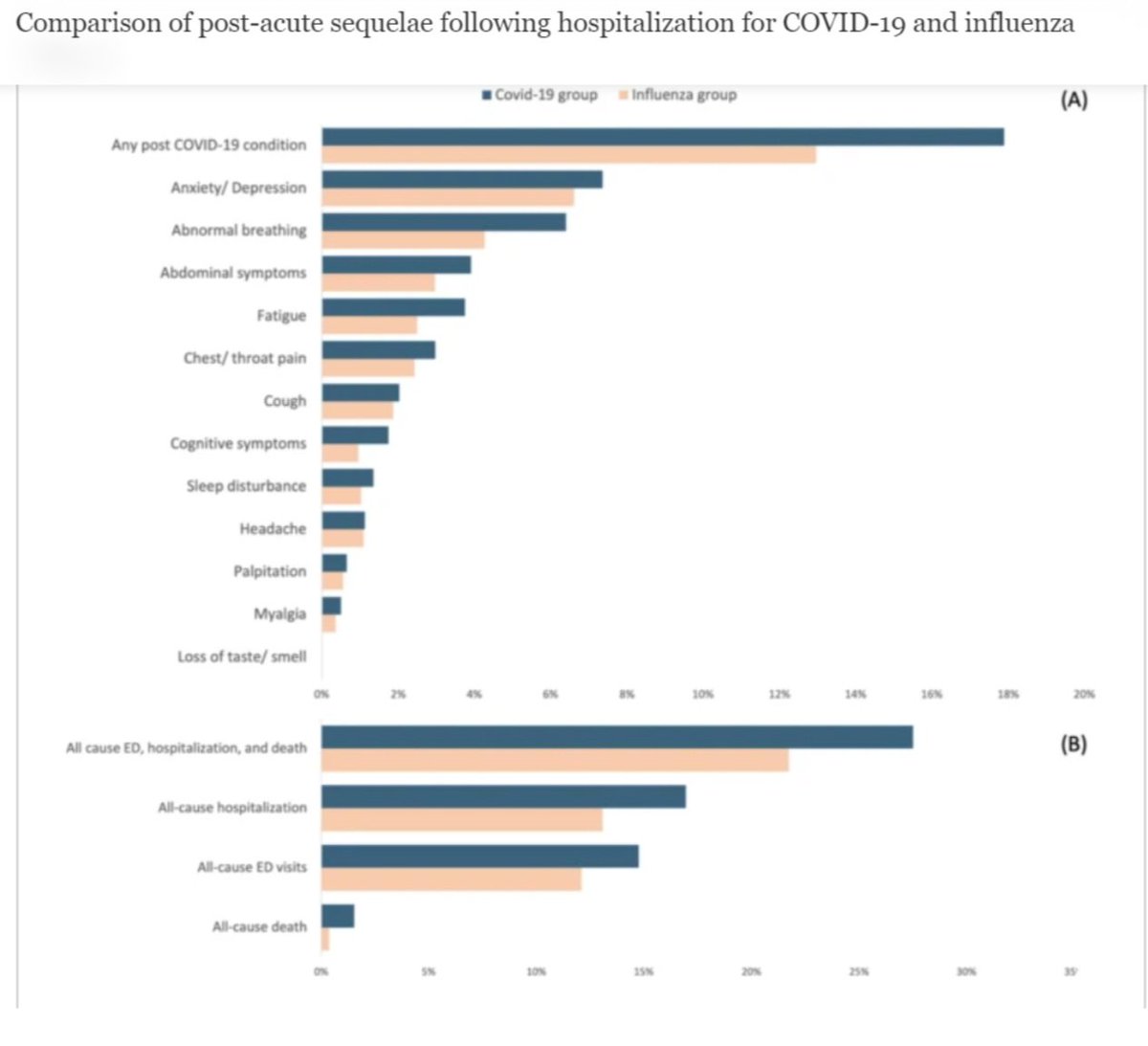
Observational studies have been mixed, but this meta-analysis of 9 such studies showed that Paxlovid treatment in the acute phase of Covid was significantly associated with a lower risk of developing LC.
h/t @JN1171 and @TogetherWeMask journalofinfection.com/article/S0163-…
h/t @JN1171 and @TogetherWeMask journalofinfection.com/article/S0163-…
But we don't really know why. Is it because it reduces risk of severe disease? Clears the virus better? Prevents progression to the inflammatory phase? Something else? We don't know because observational studies by definition aren't conclusive. We'd need an experiment to confirm.
All observational studies I've seen on this so far show either no difference or reduced risk. It's good no study has found a negative association - everything roughly points the same way. Observational studies are great to help us generate hypotheses & determine what to do next.
A clinical trial on LC prevention with antiviral treatment would have its challenges. It's unethical to withhold Paxlovid from someone who needs it, so you may need to focus on low risk people, which means leaving out some of the very populations we're concerned about.
Just 2 small examples of difficulties with clinical trials, not to mention time and expense that sometimes make them prohibitive.
For now, several observational studies do suggest that taking Paxlovid for covid may reduce the risk of LC, but more study is still needed.
For now, several observational studies do suggest that taking Paxlovid for covid may reduce the risk of LC, but more study is still needed.
If you're otherwise someone who should take Paxlovid, it's easy: you're taking it to prevent progression, hospitalization & death with this potential added benefit. If not, unfortunately I still don't think we have sufficient data to support prescribing it just for LC prevention.
We still have a lot to learn and a lot more work to do to even begin to address the increasing burden of long covid. I'm glad to see more trials being conducted and hope for more positive results soon. In the meantime, please stay safe. 🙏🏾❤️
I go over this meta-analysis as well as the recent clinical trial that did not show benefit in people who already have LC in today's briefing.
https://x.com/NohaAboelataMD/status/1800751914298261951?t=Q7dl4hFmYF0DMdDXrnZ2aA&s=19
• • •
Missing some Tweet in this thread? You can try to
force a refresh