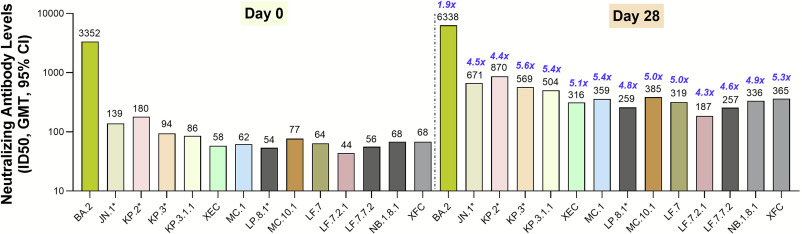
Excellent broad cross neutralization to variants with the upcoming JN.1 Novavax COVID vaccine, including some of the best responses to variants that are likely to be dominant this late fall and early winter
novavax.widen.net/s/zg79lxwknx/2…

novavax.widen.net/s/zg79lxwknx/2…

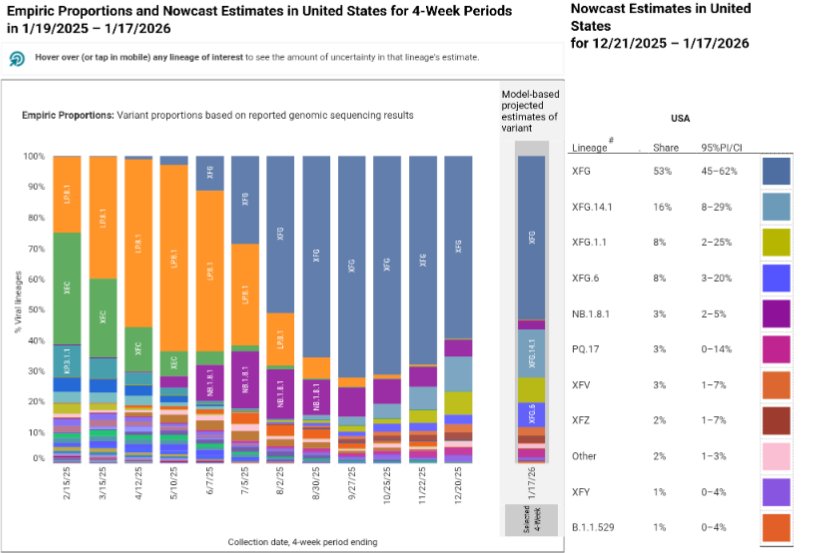
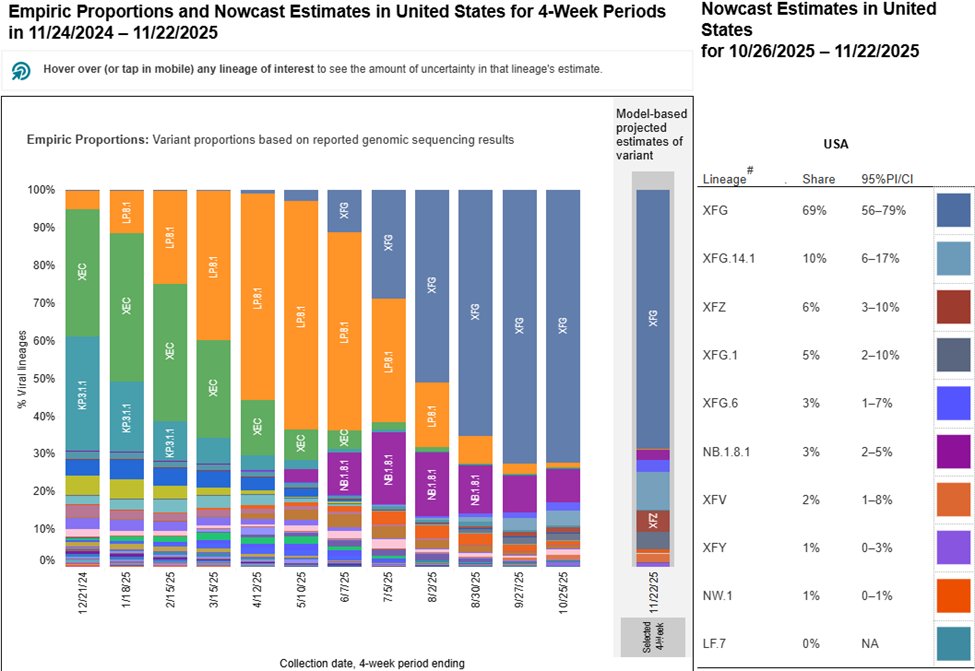
The latest CDC nowcast shows a rapid rise in KP3.1.1, which is the variant with best response to the NVX JN.1 vaccine. Others variants to keep an eye on include LB.1 (a direct JN.1 descendant) and LP.1 (KP1.1 descendant)
covid.cdc.gov/covid-data-tra…
covid.cdc.gov/covid-data-tra…

This follows an expected decline in KP.2 over the last few weeks, which is one reason why VRBPAC recommended not chasing this branch (KP.2 variant) but to target the trunk (JN.1).
https://x.com/Daniel_E_Park/status/1802177249661038747
Ultimately as the antigenic distance is very close for all major circulating variants, all vaccine options should be very good, and provide good protection against infection and severe disease (even when compared with infection-acquired/natural immunity).
cdc.gov/mmwr/volumes/7…
cdc.gov/mmwr/volumes/7…
• • •
Missing some Tweet in this thread? You can try to
force a refresh