There is a common and dangerous misconception that the JN.1 vaccines are inferior to KP.2 vaccines. In reality, JN.1 and KP.2 vaccines will both provide excellent protection, with each being slightly better in different aspects. But the experts were right to pick JN.1. 

First, a bit of background. The FDA vaccine expert committee, consisting of 14 highly experienced and accomplished vaccine experts, supported selecting JN.1, with many suggesting it would be a safer and potentially better strain to select compared w/ KP.2.
fda.gov/advisory-commi…
fda.gov/advisory-commi…
Some examples –
Dr. Berger: “I think the antigenic close relationship between JN.1 and its sublineages, and the cross-reactivity [across] KP2 and KP3, really does suggest that JN.1 is the appropriate vaccine update to be making at this time”
Dr. Berger: “I think the antigenic close relationship between JN.1 and its sublineages, and the cross-reactivity [across] KP2 and KP3, really does suggest that JN.1 is the appropriate vaccine update to be making at this time”
Dr. Wharton: “… we can't predict which variants are going to emerge... It may very well not be any of the ones that we're talking about today, but they're likely to be related to JN.1. So having a vaccine that's the trunk of the tree rather than the branches makes sense…”
Dr. Chatterjee: “I would say that a JN.1 is a reasonable strain to include… we're not going to be trying to chase variants”. Dr. Gans: “I think if it goes in a different direction, having a JN.1 would allow for some protection in a different direction as well.
Dr. Gellin: “the trunk of the tree [JN.1] probably is our best bet for now” and Dr. Nelson: “at this time of the evolution of the vaccine, and the comfort from the neutralization data presented, that JN.1 is a natural and obvious choice going forward”
FDA CBER director Dr. Marks offered KP.2 could be preferable because: “do we think there's some possibility that KP2 and KP3 are potentially going to evolve back closer to JN.1… And if this evolves further in the fall, will we regret not having been a little bit closer?”
This argument is a very common misconception in the general public, and even among some scientists.
Specifically, the vaccine experts knew the variants circulating in Fall/Winter 2024 would be just as (or more) likely to be JN.1 descendants, and not a KP.2 descendant. Evolution is rarely linear, and they did not want to chase a variant and get stuck at the end of a dead branch.
E.g. If picking a person who will best genetically represents a large extended family in 50 yrs, do you pick a parent, or one of the kids? It’s possible a kid you pick will have many kids and be a better match, but it’s safer to pick the parent (even if they’re no longer around)
This is exactly what we see now. As you can see, both JN.1 and KP.2 are gone. Critically, KP.2 descendants are rare, and the bulk of infections are JN.1 descendants, with KP.3.1.1 being dominant.
covid.cdc.gov/covid-data-tra…
covid.cdc.gov/covid-data-tra…
What about KP.3? A common misconception is that KP.3 descended from KP.2 (due to numbers being sequential). But KP.3 is a direct JN.1 descendant, not at KP.2 descendant. They do share some key mutations, and this could suggest KP.2 could be a better match than JN.1
However, the data shows better coverage for KP.3 using a JN.1 target from one manufacturer, while the other saw KP.2 as better. This is a critical reason why last month (July), the EMA (EU) expert committee decided to stay with JN.1 based on recent data
ema.europa.eu/en/documents/o…
ema.europa.eu/en/documents/o…

How about KP.3.1.1? While KP.3.1.1 has some mutations in common with KP.2, the S31 deletion may have changed the conformation (structure) or stability of the spike, altering the impact of the mutations shared with KP.2
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
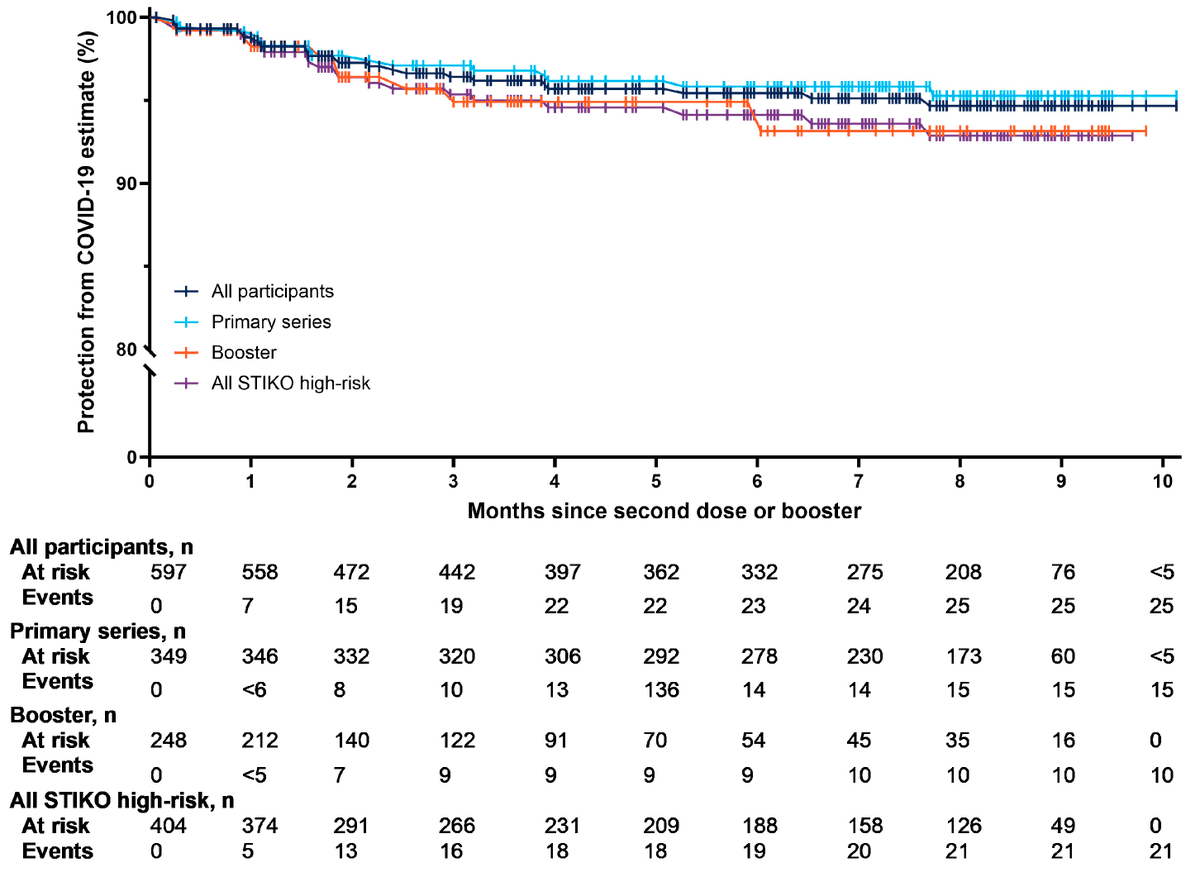
As a result, the are indications that JN.1 provides an excellent response to KP.3.1.1, both from sera (none at LOD / low response) and early manufacturer data (high nAbs)
thelancet.com/journals/lanin…
thelancet.com/journals/lanin…
https://x.com/Daniel_E_Park/status/1821552971110383622

Experts w/ experience working with strain selection have learned from experience. Viral evolution does not typically proceed linearly, but tends to circulate around a nexus that balances immune evasion and infectivity – JN.1 is more central.
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…

Ultimately, JN.1 and KP.2 are very similar and either will provide excellent protection for this fall and winter. But the FDA decision to override the VRBPAC recommendations made some other collateral damage.
The experts noted that JN.1 may also allow for earlier introduction since it had been in development longer. This could allow FDA to approve ahead of an anticipated August surge. They were also right on that front
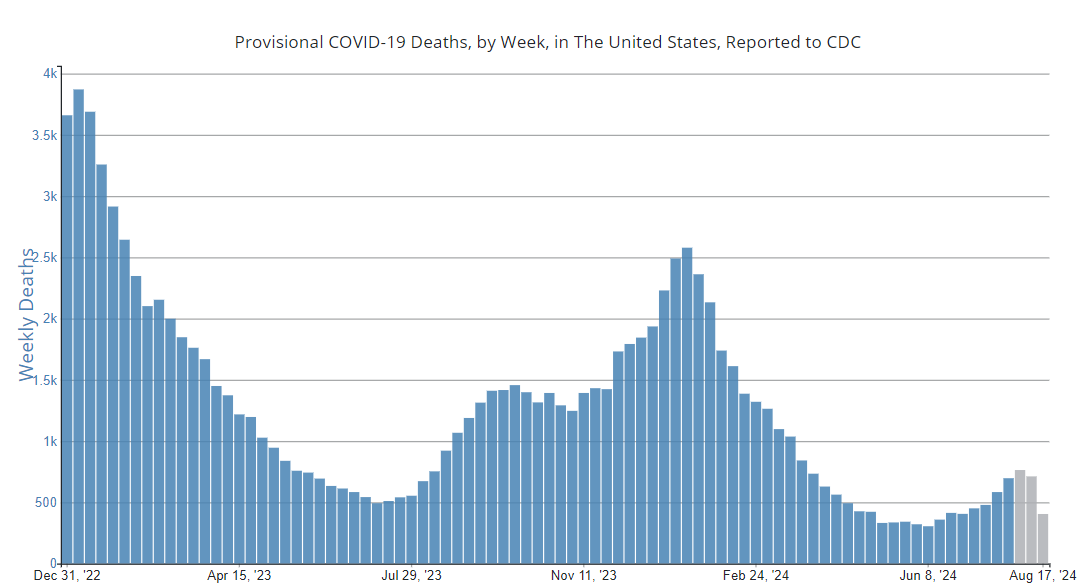
The FDA heard the “loud and clear” message about JN.1, but instead moved ahead with recommending KP.2 “if feasible”. The KP.2 approvals came just after the August surge the VRBPAC warned of. And Novavax JN.1 (w/ excellent match to dominant KP.3.1.1) is still awaiting FDA approval
As has happened repeatedly, experts were ignored, potentially leading to thousands of preventable infections and deaths.
This misconception about JN.1 inferiority may cause many more deaths via hesitancy, since globally, almost all countries will only have JN.1 vaccines. The public health messaging must be that both JN.1 and KP.2 are excellent options. Full stop.
• • •
Missing some Tweet in this thread? You can try to
force a refresh