1/ The mRNA platform must not be a consideration for humans animals or plants! The Lipid Nanoparticles alone are a deal breaker, period! 🧵 

2/ Risk/benefit analysis is key in all medical intervention decisions.
3/ Don’t fall for “safe and effective” without full analysis.
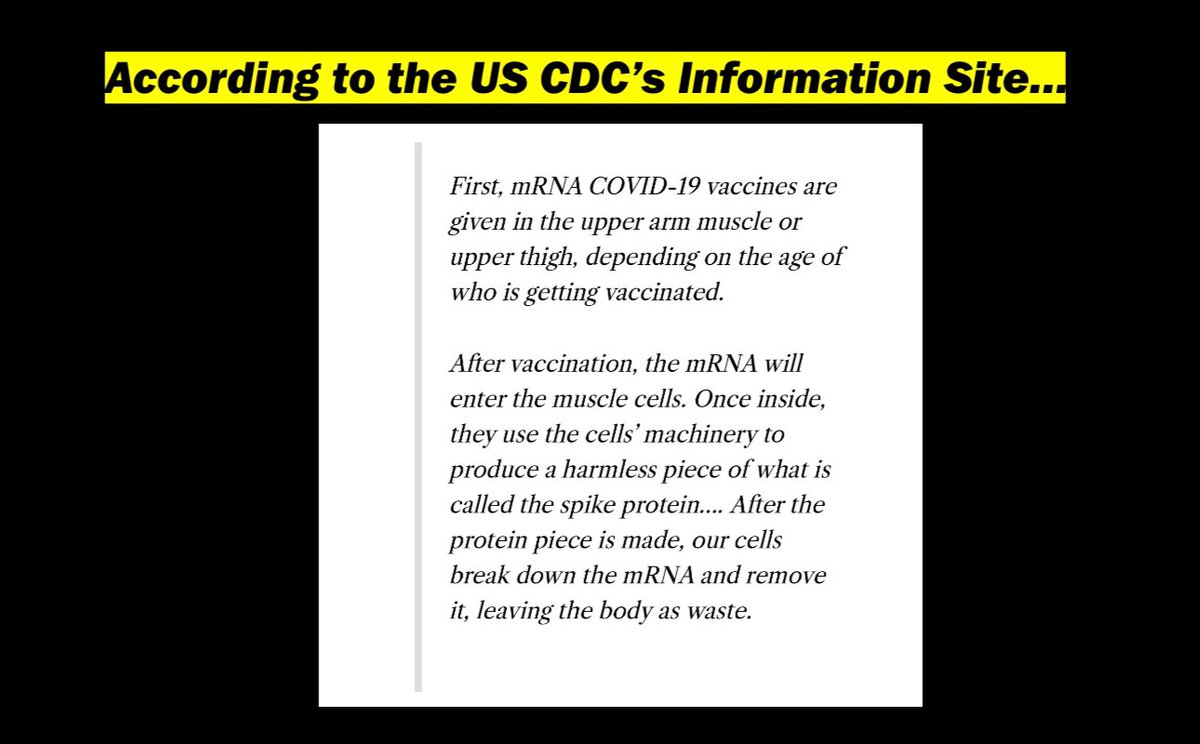
4/ Such decisions require informed consent and transparency. This, from the @CDCgov is medical disinformation (yes I’m using their own terms).
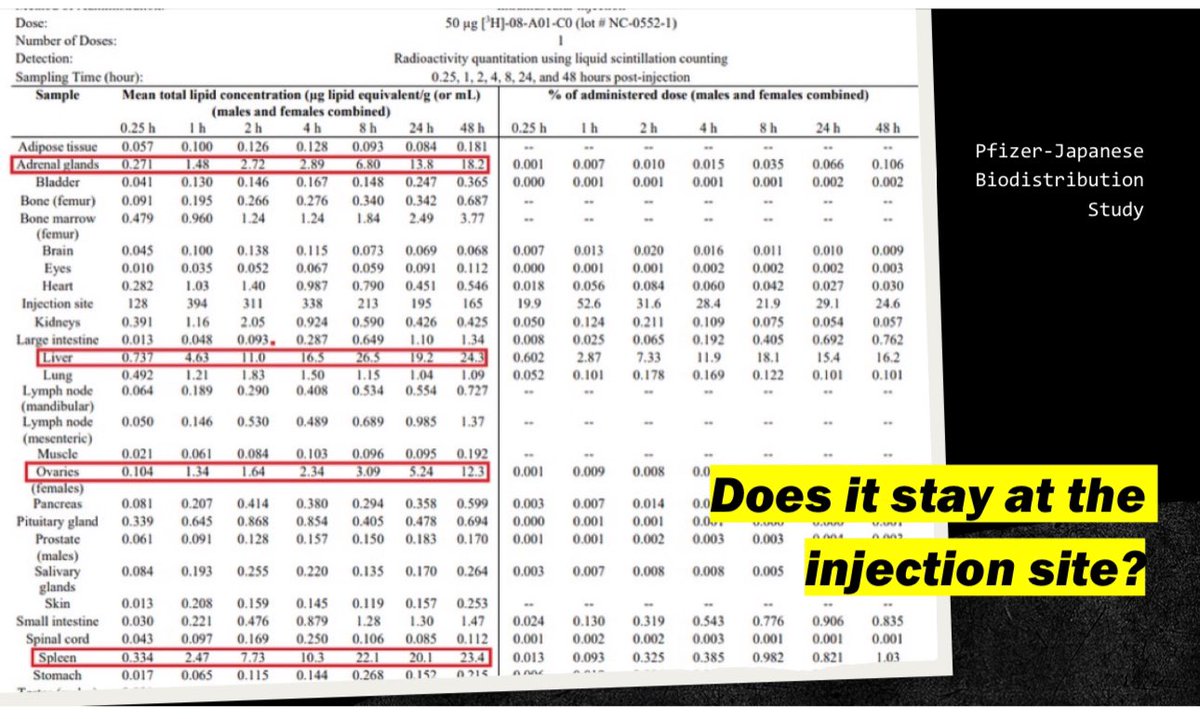
5/ They ended the biodistribution studies before Cmax was reached. Nothing peaked yet before study was ended.
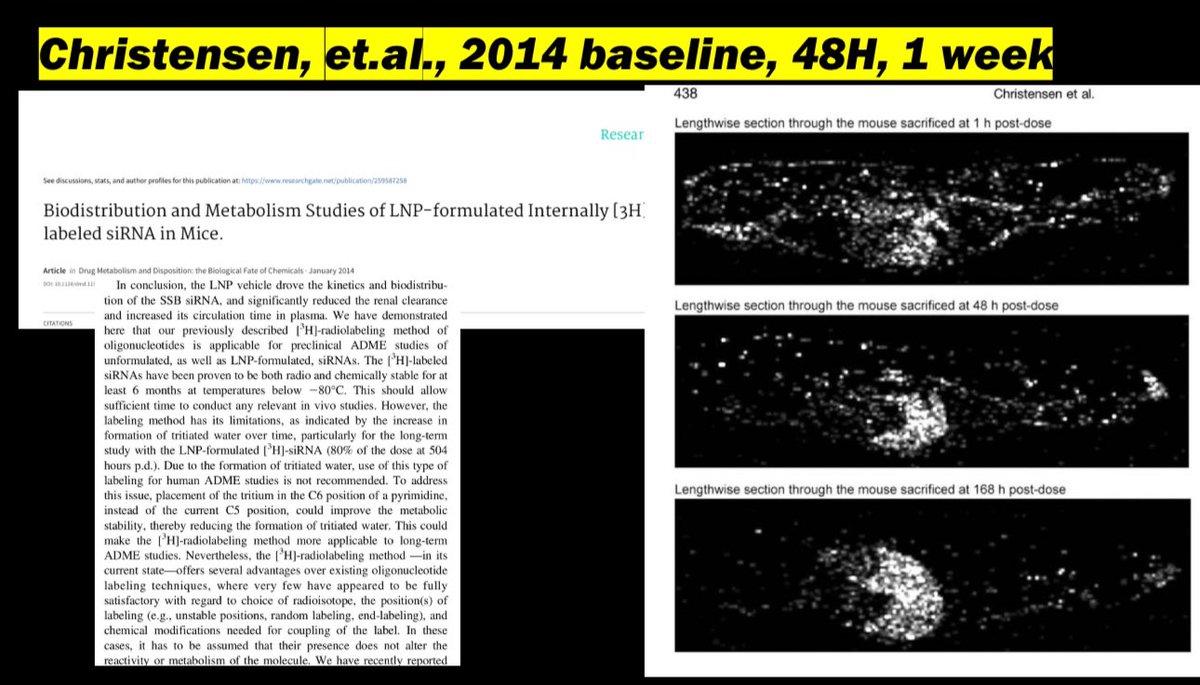
6/ They knew back in 2014 that the accumulation increases and continues far beyond their study duration.
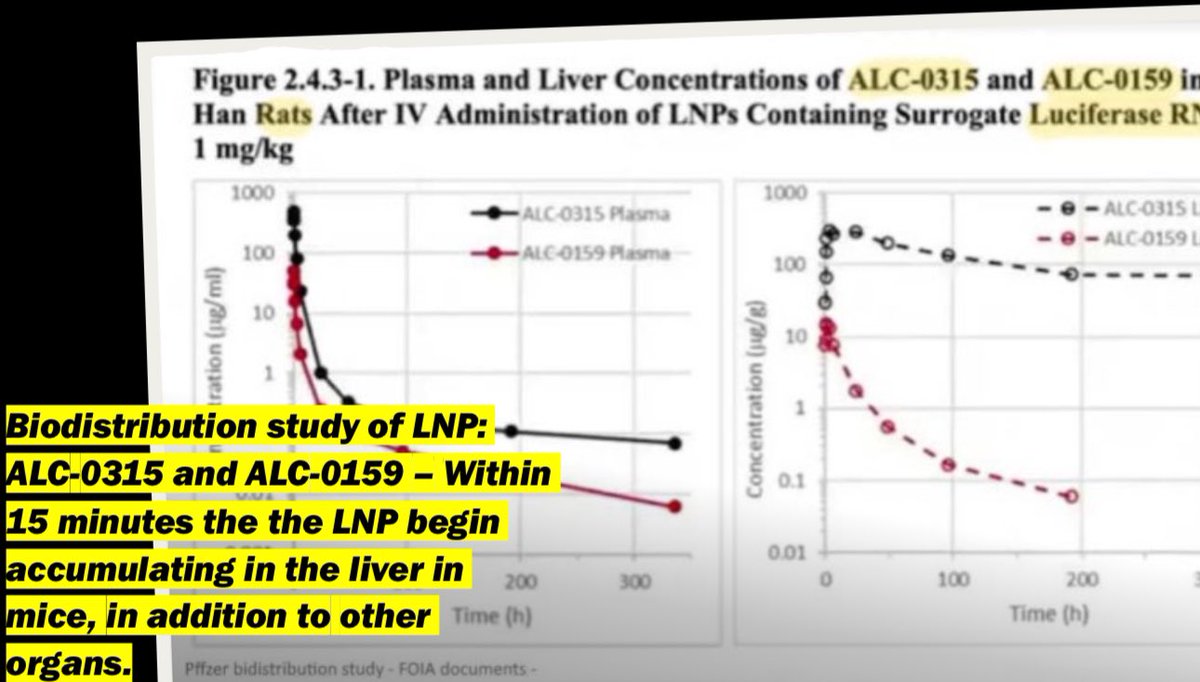
7/ The very same LNPs in the liver within 15m.
8/ More definitive evidence that the CDC was not honest in their representation of the LBP gene therapy.
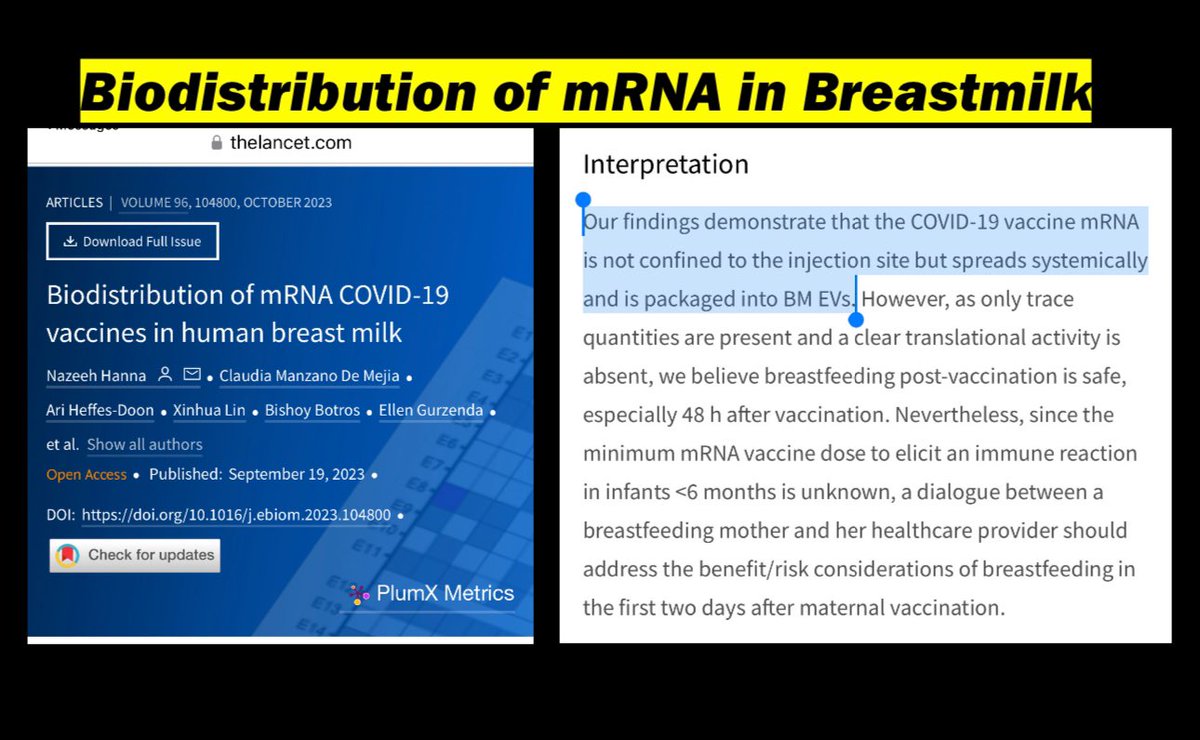
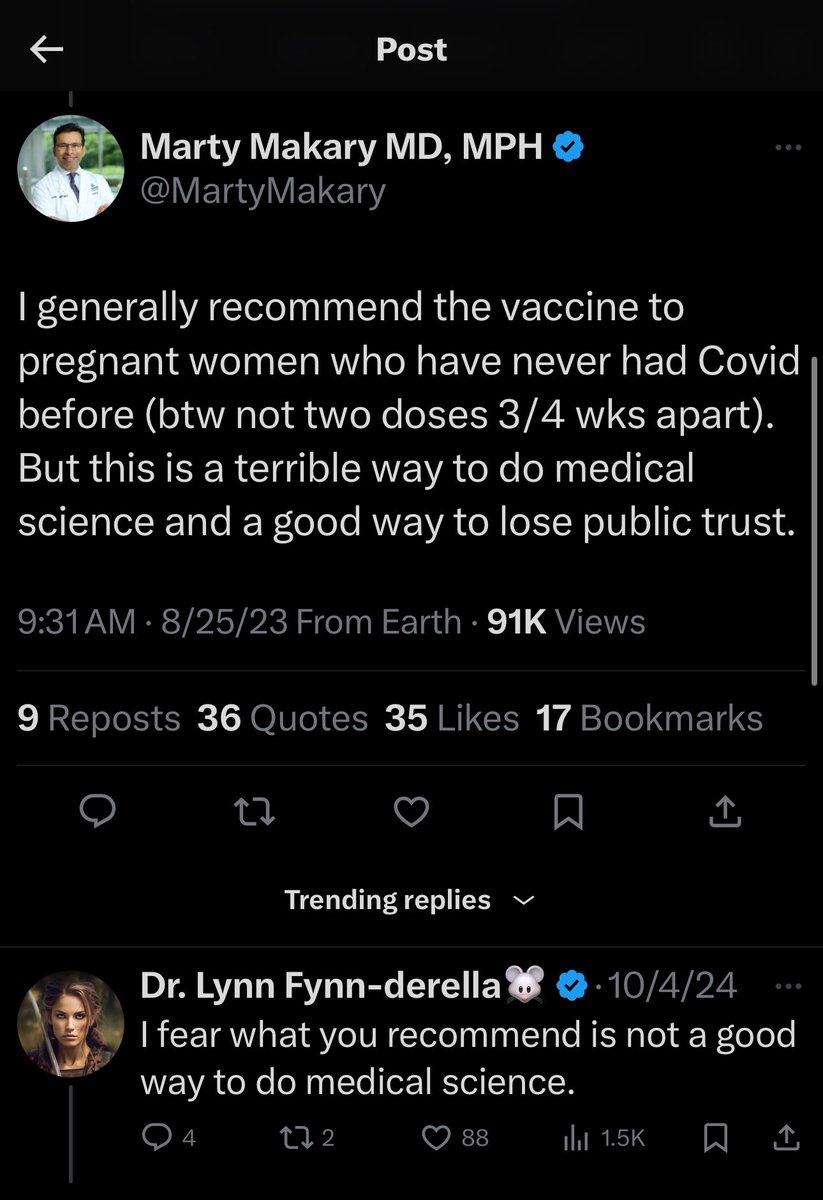
9/ the LNP/modmRNA transfer through breast milk, yet as late as 2023 “experts” recommend it during pregnancy!
10/ They knew this going back to 2010.
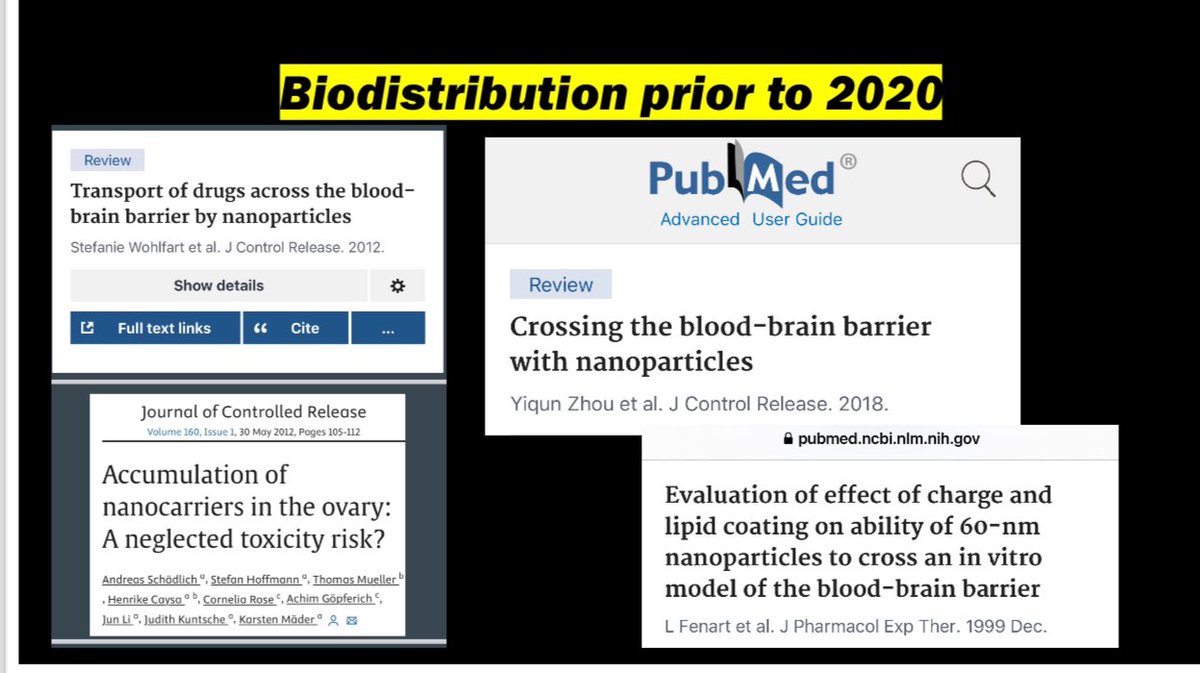
11/ The LNP carriers can reach the trophoblasts on their own and induce apoptosis.

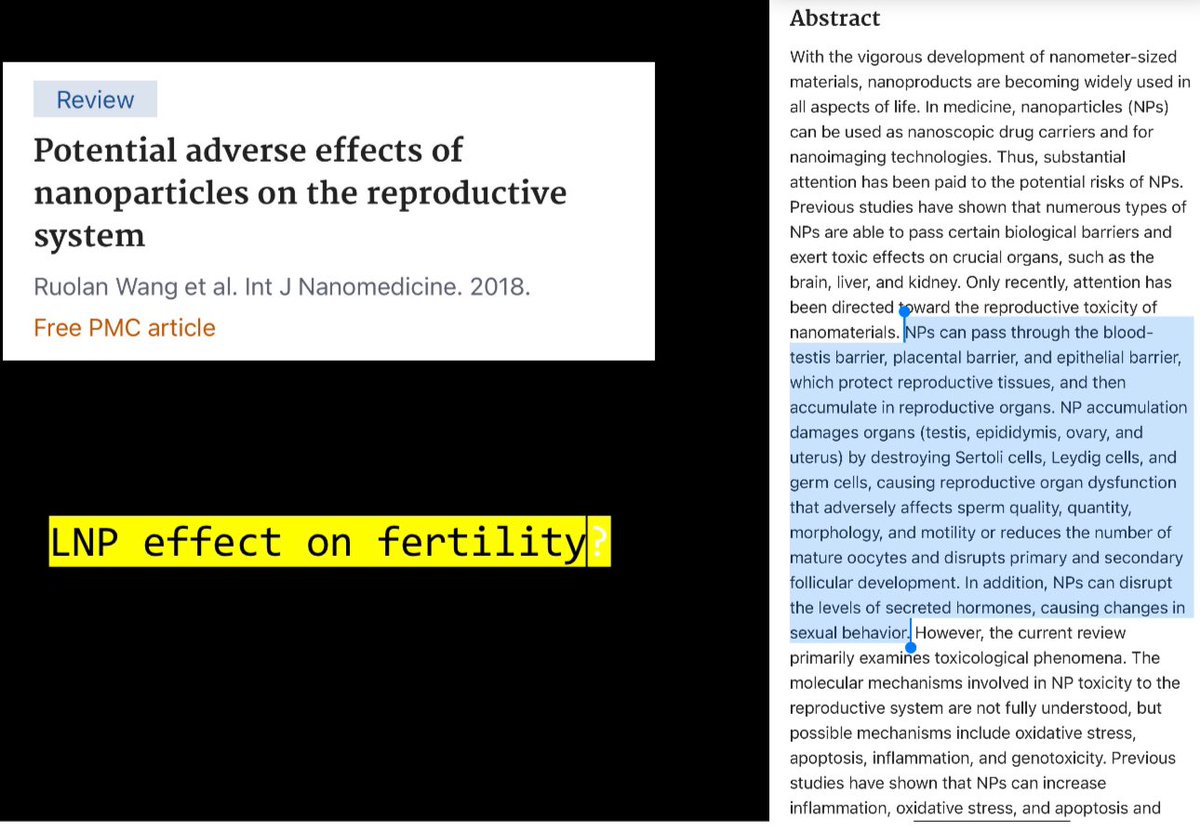
12/ Just the LNPs alone wreak havoc on the reproductive drive system. Morexreas ns why this platform in healthies is a hard pass!
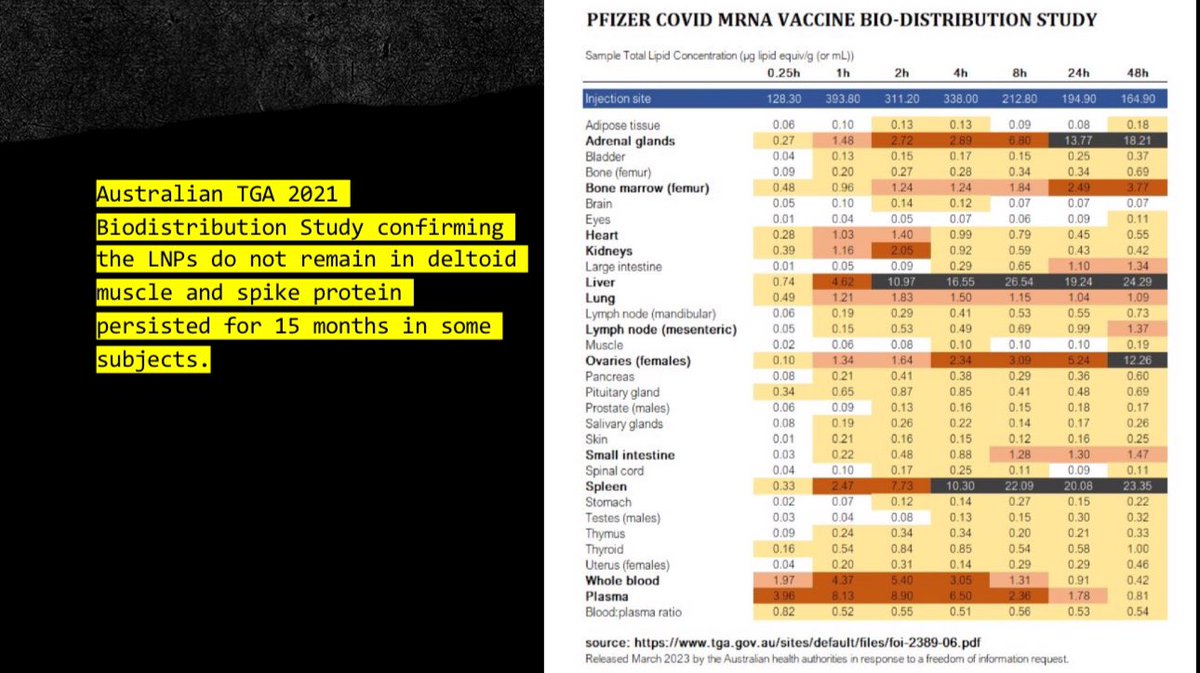
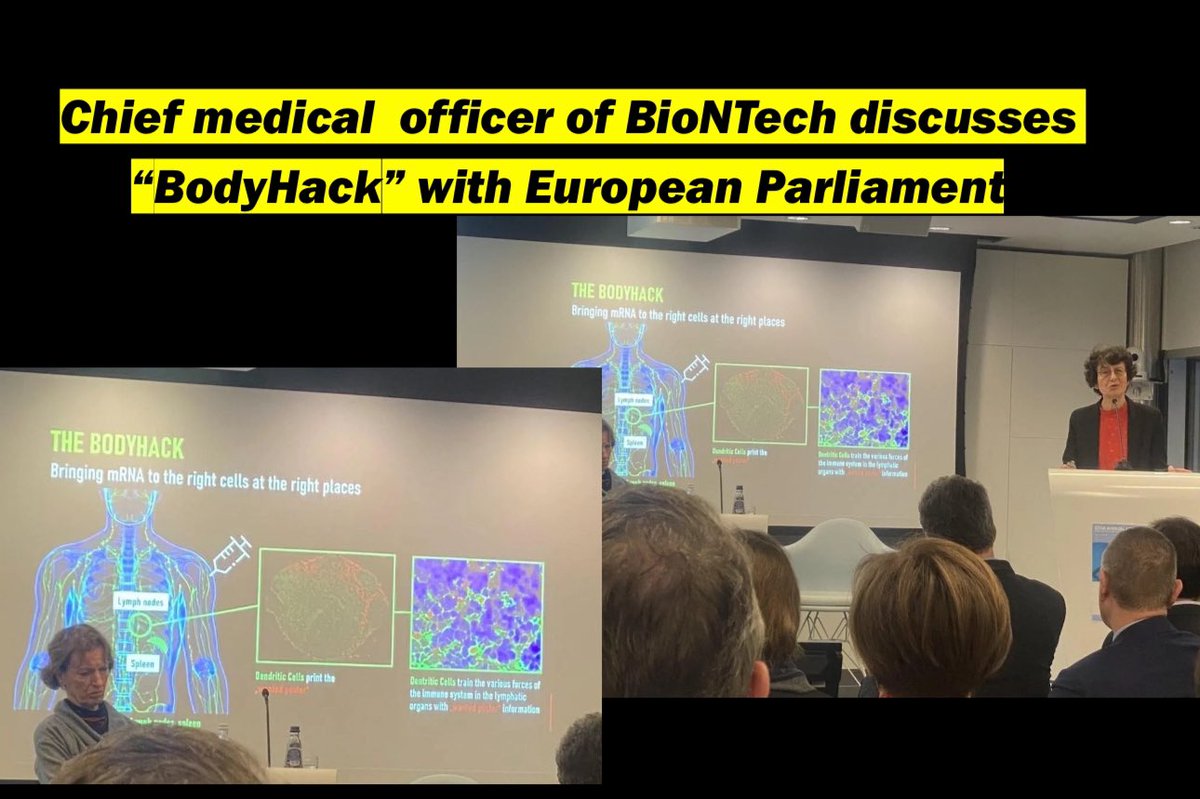
13/ they knew it wouldn’t stay at the injection site, and even called it a #bodyhack and described it as a “feature”.
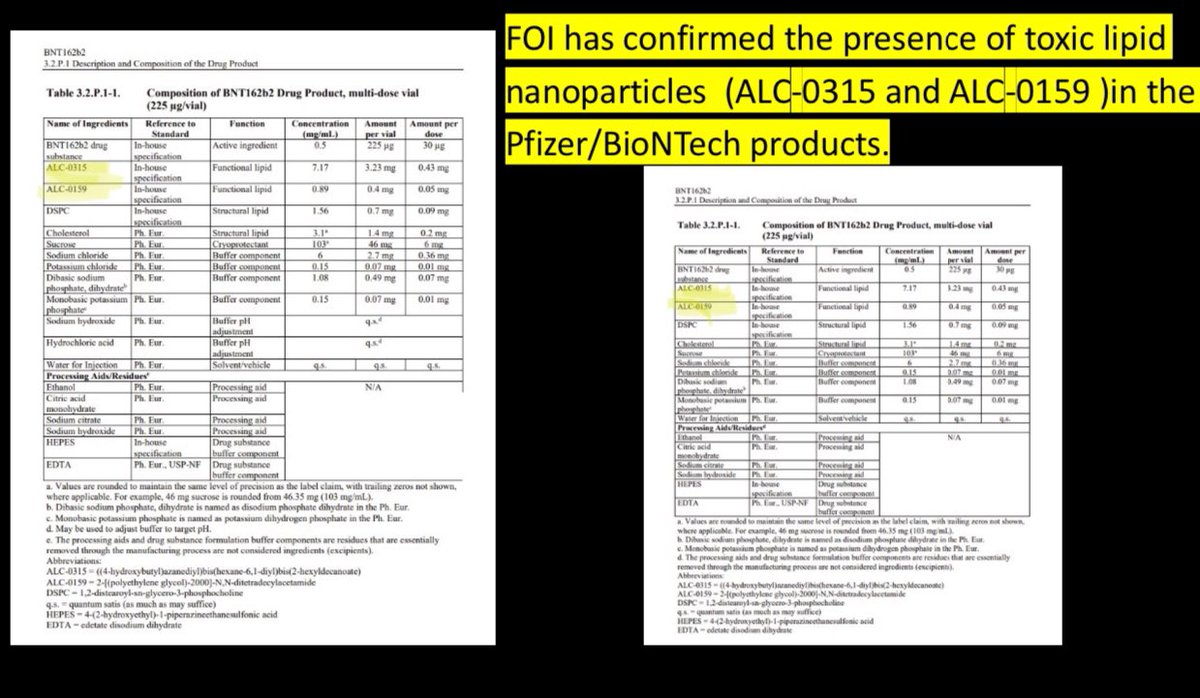
14/ we know these particles core are the ones used in Pfizer.
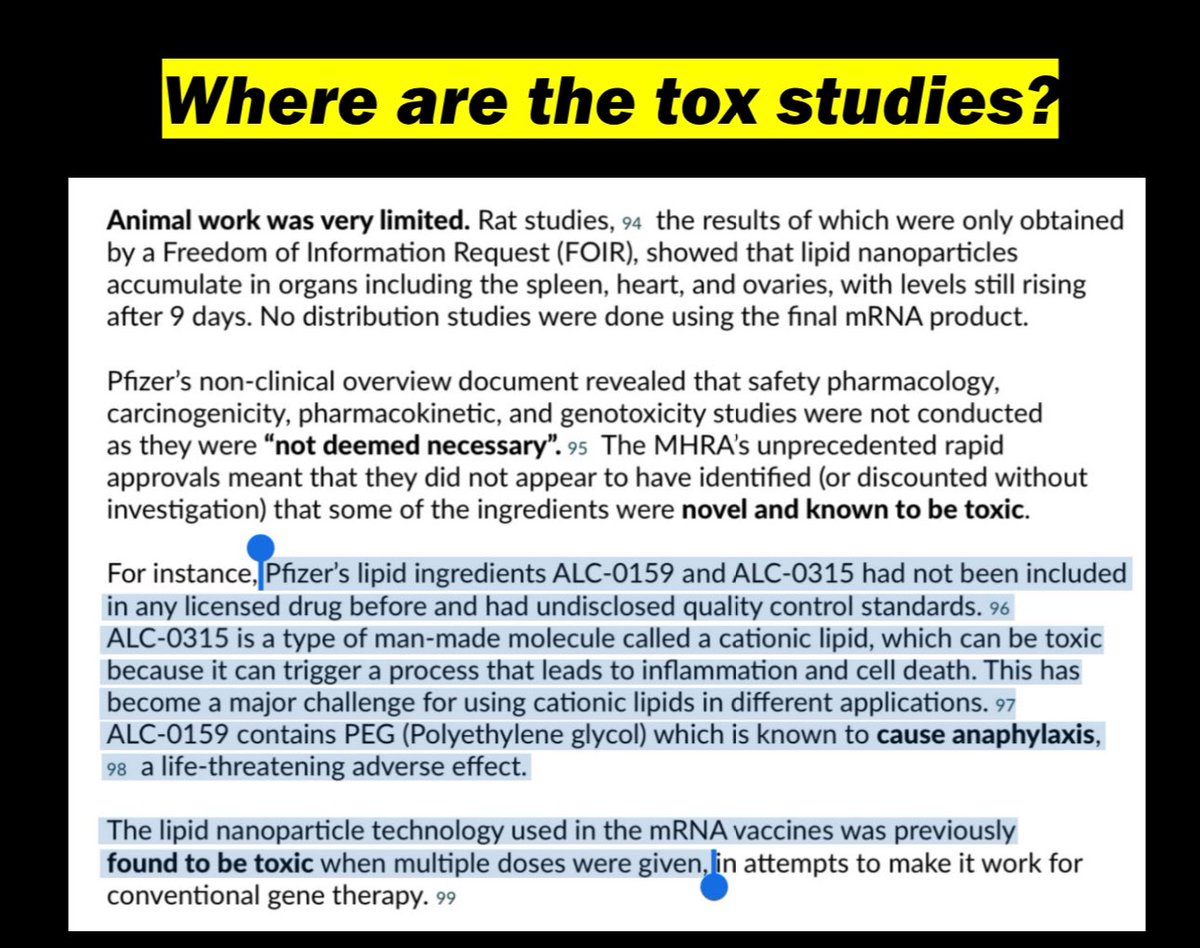
15/ where are the tox studies, and teratogenicity, carcinogenicity, genotox studies?
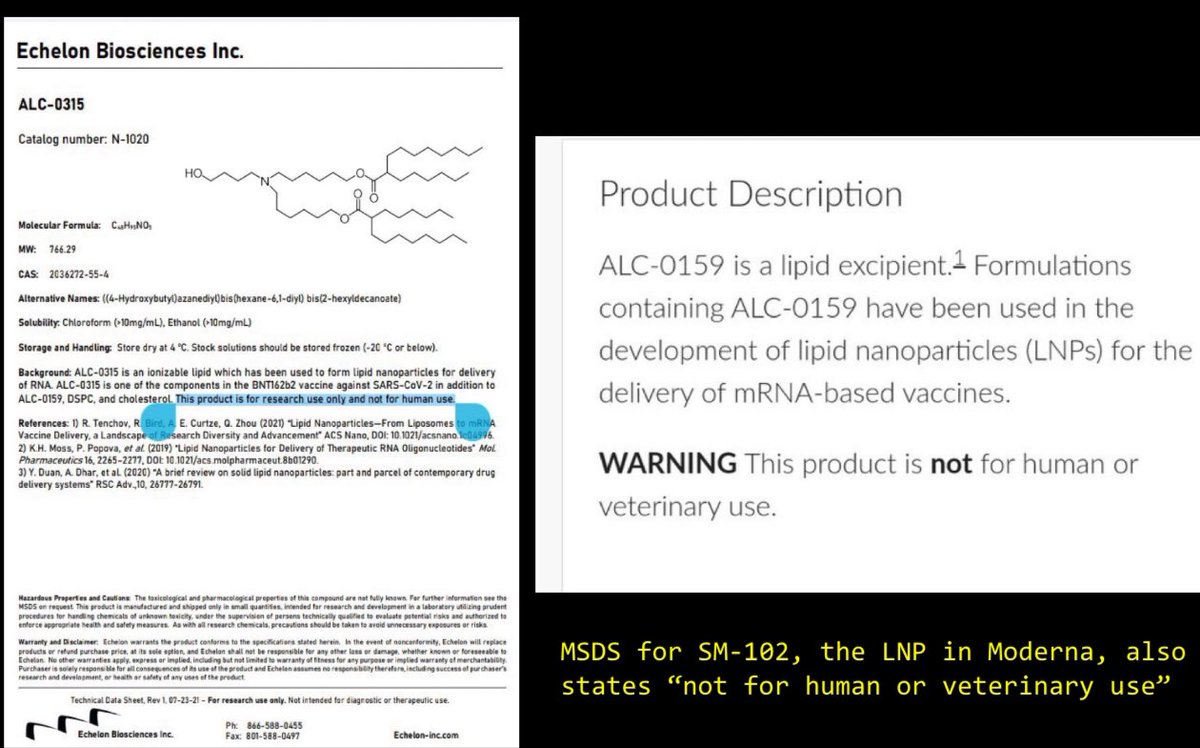
16/ Not for human use, until an #EUA allows more lax regulations to experiment on the once-healthy masses.
17/ and they got away with ignoring their x studies because they classified LNPs as excupients. I even argued with Paul Offit about this distinction, but he is clueless about CMC, and pushed a false narrative.

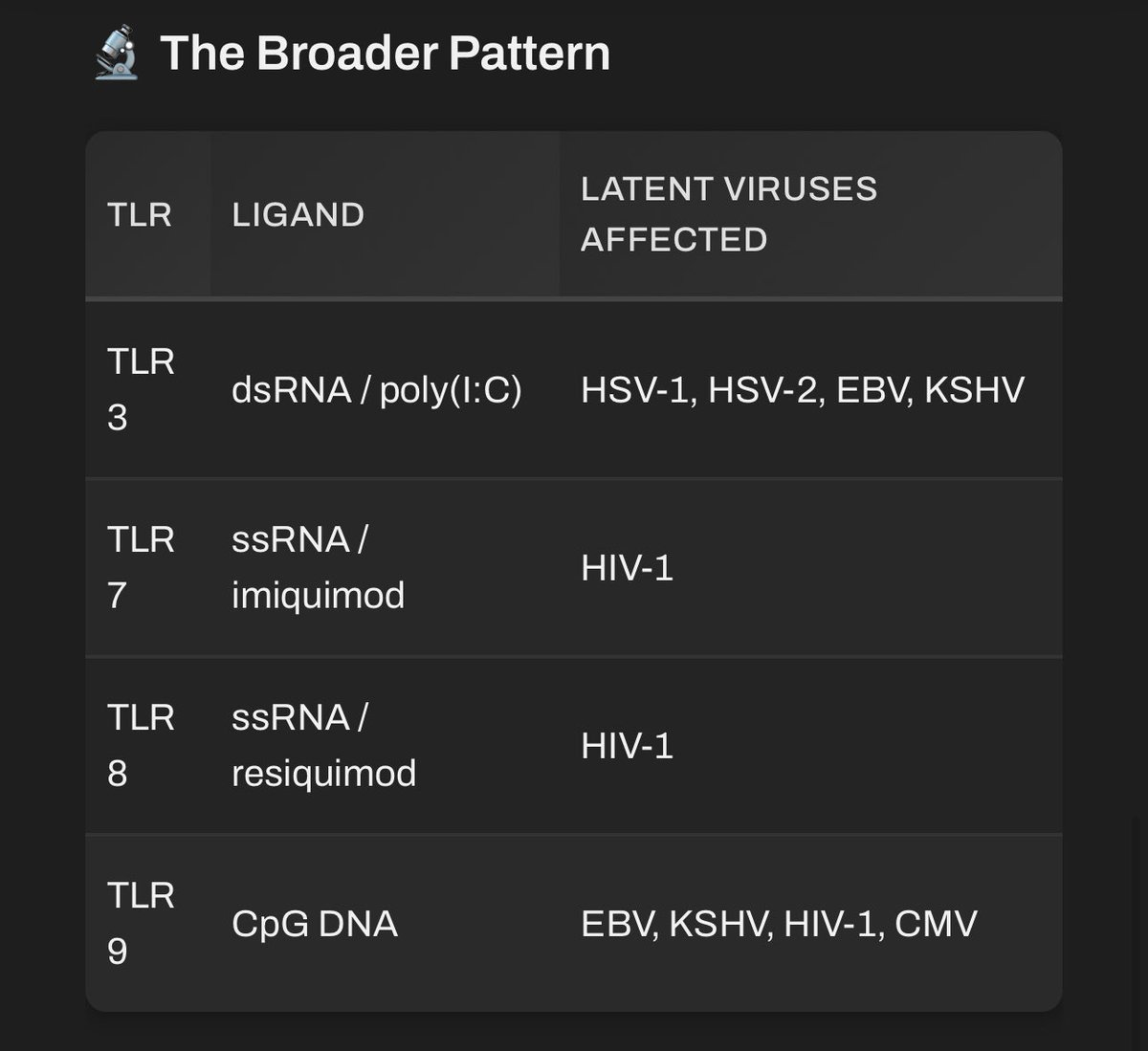
18/ They cause universal inflammation. So many implications of harm.
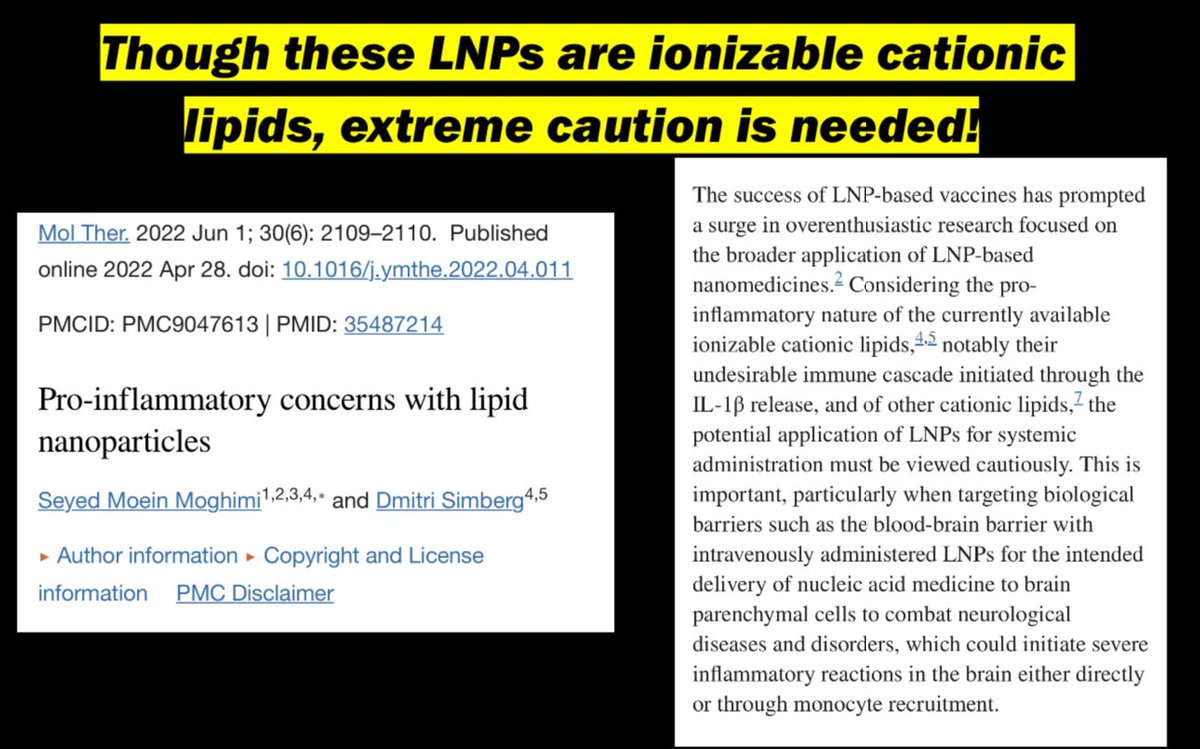
19/ Multiple pathway triggers anyone?

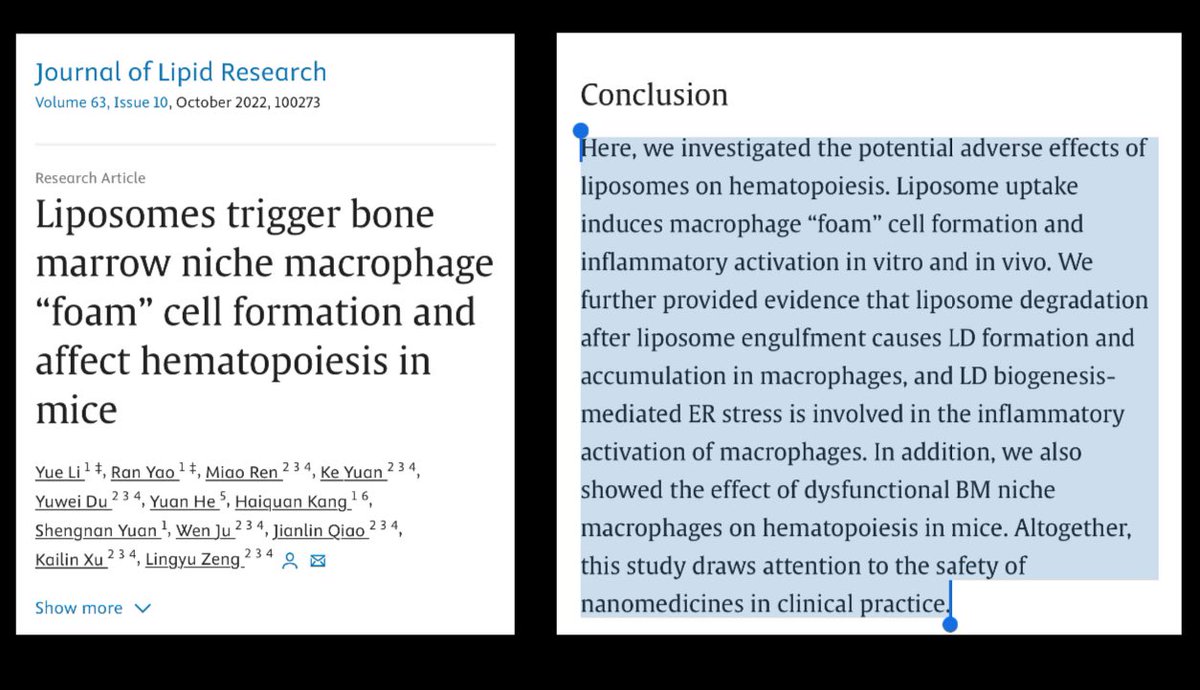
20/ LNPs alone triggering foam cells? What implications do they have on platelet, or blood cell formation?
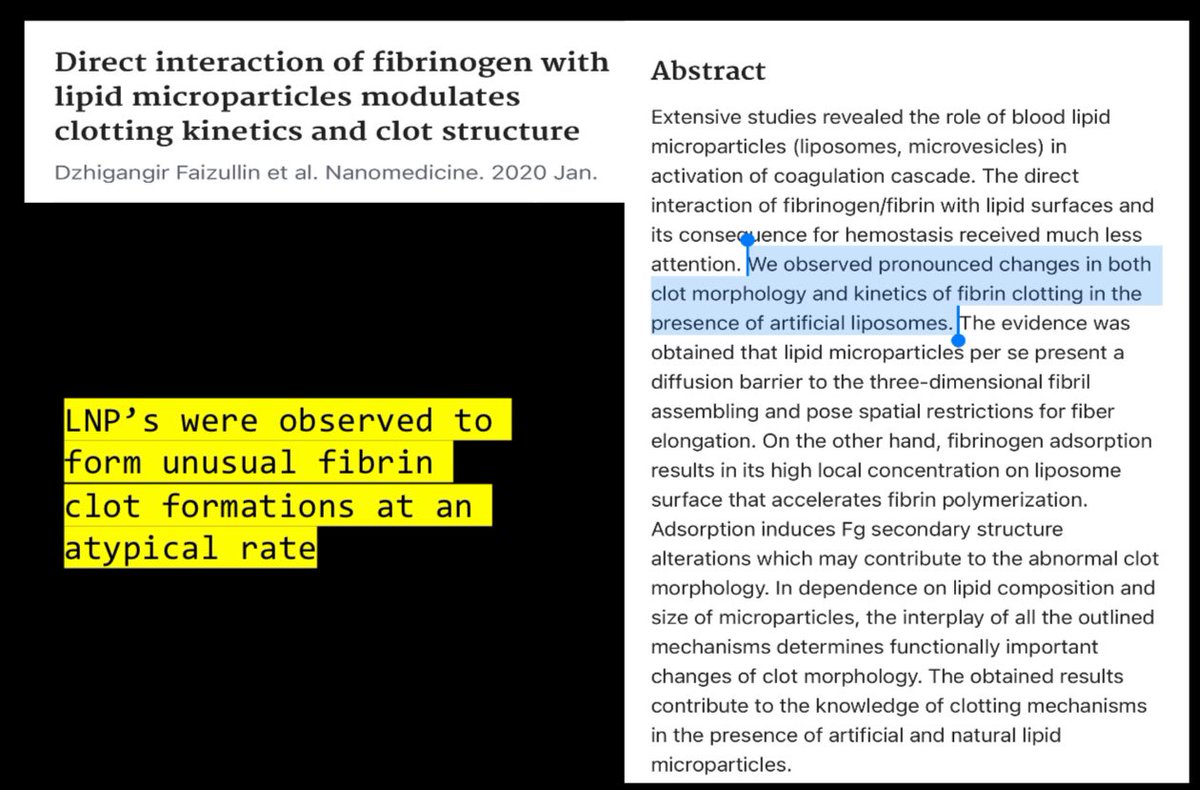
21/ the carrier alone modulates clot formation. What could go wrong with this platform?
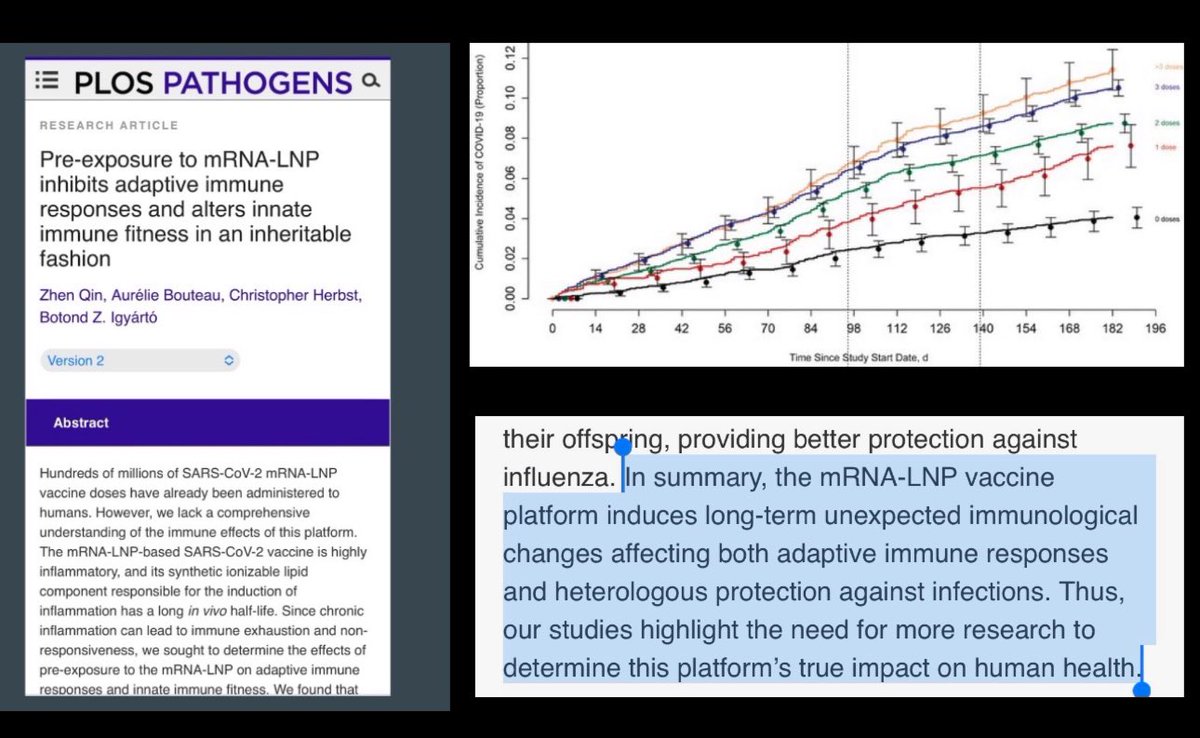
22/ This platform alters both innate and adaptive immunity! IgG4 makes recipient more prone to constant infection.
23/ Don’t get me started on zeta potential!

24/ When others know it’s dangerous and discontinued development, maybe it should be an indication it may be harmful?

25/25
Was this a good idea to roll out to the world’s population for an infection that they couldn’t even find enough mortality to properly study necessity of such an intervention? I fear an entire generation plus will feel the consequences of such an irresponsible measure.
Was this a good idea to roll out to the world’s population for an infection that they couldn’t even find enough mortality to properly study necessity of such an intervention? I fear an entire generation plus will feel the consequences of such an irresponsible measure.
Weird autocorrect (excipients)
Tox studies. (Autocorrect hates science almost as much as our captured agencies do.)
Great video from my friend GB #Narf
https://twitter.com/Nicolina0815/status/1865848482889597334
More reasons …. Autocorrect




28) Properties of LNPs as an abrasive can also cause physical damage not just biochemical. pubs.rsc.org/en/content/art…
29) pubs.acs.org/doi/10.1021/ac…
“Furthermore, LNPs can transfect a variety of immune cells in the bloodstream, such as dendritic cells and macrophages [25]. They can also exit the circulation through fenestrated endothelium or transcytose into different tissues depending on the route of administration and the specific LNP formulation, then circulate there as they are exocytosed after initial cellular uptake [12]. Lipid nanoparticles also induce oxidative stress, which can enhance the release of exosomes (containing the cargo and cationic ionizable lipids) into the external environment and their circulation throughout the body [26]. For example, Wei et al. compared four LNP formulations, Onpattro-like (DI-8), Moderna, and Pfizer/BioNTech-like, and observed differences in systemic leakage of the labelled mRNA into the circulation at 12 hours. Less leakage was observed with the more stable Onpattro-like formulation (13.9%) than with the Moderna formulation (31.4%). Based on these observations and others (Ren, Kent, Maugeri, 2019), we propose that LNPs exhibit various levels of uptake, systemic circulation, transfection, and exocytosis that depend on the formulation, route, and other factors, which occur simultaneously and are overlapping in nature. Moreover, Balcorta et al. (Nano Lett., 2025, 25, 7682–7689) demonstrated that conventional radiotracing and fluorescent labeling approaches lack the subcellular resolution required to map LNP distribution accurately, and introduced peptidebased tags that enable reliable visualization of LNP trafficking within cells and tissues.”
pubs.acs.org/doi/10.1021/ac…
“Furthermore, LNPs can transfect a variety of immune cells in the bloodstream, such as dendritic cells and macrophages [25]. They can also exit the circulation through fenestrated endothelium or transcytose into different tissues depending on the route of administration and the specific LNP formulation, then circulate there as they are exocytosed after initial cellular uptake [12]. Lipid nanoparticles also induce oxidative stress, which can enhance the release of exosomes (containing the cargo and cationic ionizable lipids) into the external environment and their circulation throughout the body [26]. For example, Wei et al. compared four LNP formulations, Onpattro-like (DI-8), Moderna, and Pfizer/BioNTech-like, and observed differences in systemic leakage of the labelled mRNA into the circulation at 12 hours. Less leakage was observed with the more stable Onpattro-like formulation (13.9%) than with the Moderna formulation (31.4%). Based on these observations and others (Ren, Kent, Maugeri, 2019), we propose that LNPs exhibit various levels of uptake, systemic circulation, transfection, and exocytosis that depend on the formulation, route, and other factors, which occur simultaneously and are overlapping in nature. Moreover, Balcorta et al. (Nano Lett., 2025, 25, 7682–7689) demonstrated that conventional radiotracing and fluorescent labeling approaches lack the subcellular resolution required to map LNP distribution accurately, and introduced peptidebased tags that enable reliable visualization of LNP trafficking within cells and tissues.”
pubs.acs.org/doi/10.1021/ac…
30)
Lipid nanoparticles (LNPs) are a critical structural element of modern mRNA therapeutics, including COVID‑19 modRNA vaccines. Each formulation is a multicomponent system in which the LNP serves not as a passive carrier but as an active, biointeractive entity whose ionizable lipids engage directly with cellular membranes. Current evidence from cellular, transcriptomic, and proteomic analyses indicates that LNPs, with or without active mRNA cargo, alter transcriptomic programs and protein expression. This suggests that, even during uptake and interaction with the membrane (transfection), the membrane serves as an initial site for inflammatory, detoxifying, and stress responses. Simultaneously, pathways involved in fat metabolism and detoxification are affected, such as the peroxisome proliferator-activated receptor γ (PPARγ) and cytochrome P450 (CYP) enzyme systems. We believe that the phosphatidylinositol (PI) cycle is the initial point for these disorders. This cycle regulates both organelle trafficking and membrane restructuring following endocytic processes, including macropinocytosis. When this cycle is disrupted, membrane restructuring and organelle dysfunction occur, triggering downstream signaling cascades such as nuclear factor kappa-B (NF- κB), mitogen-activated protein kinases (MAPKs), Janus kinase–signal transducer (JAK-STAT) pathways, and mechanistic target of rapamycin (mTOR) complexes. Transfection with LNPs may induce a systemic condition we call lipid-nanoparticle-driven membrane dysfunction (L‑DMD), where transfection results in broader dysregulation of cellular communication, stress response, and energy balance. This hypothesis-driven review offers a mechanistic foundation for understanding the diffuse, often enduring, biological effects observed after exposure to messenger RNA LNP formulations. It highlights a needed perspective at the intracellular level and within systems biology.
preprints.org/manuscript/202…
Lipid nanoparticles (LNPs) are a critical structural element of modern mRNA therapeutics, including COVID‑19 modRNA vaccines. Each formulation is a multicomponent system in which the LNP serves not as a passive carrier but as an active, biointeractive entity whose ionizable lipids engage directly with cellular membranes. Current evidence from cellular, transcriptomic, and proteomic analyses indicates that LNPs, with or without active mRNA cargo, alter transcriptomic programs and protein expression. This suggests that, even during uptake and interaction with the membrane (transfection), the membrane serves as an initial site for inflammatory, detoxifying, and stress responses. Simultaneously, pathways involved in fat metabolism and detoxification are affected, such as the peroxisome proliferator-activated receptor γ (PPARγ) and cytochrome P450 (CYP) enzyme systems. We believe that the phosphatidylinositol (PI) cycle is the initial point for these disorders. This cycle regulates both organelle trafficking and membrane restructuring following endocytic processes, including macropinocytosis. When this cycle is disrupted, membrane restructuring and organelle dysfunction occur, triggering downstream signaling cascades such as nuclear factor kappa-B (NF- κB), mitogen-activated protein kinases (MAPKs), Janus kinase–signal transducer (JAK-STAT) pathways, and mechanistic target of rapamycin (mTOR) complexes. Transfection with LNPs may induce a systemic condition we call lipid-nanoparticle-driven membrane dysfunction (L‑DMD), where transfection results in broader dysregulation of cellular communication, stress response, and energy balance. This hypothesis-driven review offers a mechanistic foundation for understanding the diffuse, often enduring, biological effects observed after exposure to messenger RNA LNP formulations. It highlights a needed perspective at the intracellular level and within systems biology.
preprints.org/manuscript/202…
31) LNP database
https://twitter.com/Guillau13441190/status/2004286059602235723
Autocorrect hates me lol
• • •
Missing some Tweet in this thread? You can try to
force a refresh