
Novavax Availability Update 📢
Costco in Little Rock, AR has reportedly confirmed that they'll have Novavax stock in place by September.
My gut feeling is that this is much closer to the timeline we'll end up seeing for most stores instead of July/August.
Here's why. 🧵
Costco in Little Rock, AR has reportedly confirmed that they'll have Novavax stock in place by September.
My gut feeling is that this is much closer to the timeline we'll end up seeing for most stores instead of July/August.
Here's why. 🧵
https://twitter.com/depayser/status/1933247698292863022
In 2024, the first CVS I heard of that had received their stock was in Pittsfield, MA on September 9.
For Costco, it was in Limerick/Sanatoga, PA on September 13.
For Costco, it was in Limerick/Sanatoga, PA on September 13.
https://x.com/Friesein/status/1834619489712816398
Prior to that, the national Costco distribution center had received their stock on September 10, and they began shipping to stores shortly afterwards.
https://x.com/Friesein/status/1833996441615765511
There's been confusion on the distribution timeline of Novavax this year. This is the first year Sanofi will handle distribution, so there may be hiccups.
Or, perhaps Sanofi will handle distribution even better than Novavax. The bar is fairly low.
Or, perhaps Sanofi will handle distribution even better than Novavax. The bar is fairly low.
https://x.com/Friesein/status/1932791957404667998
There's one thing that has to happen before any pharmacy in the US can administer Novavax:
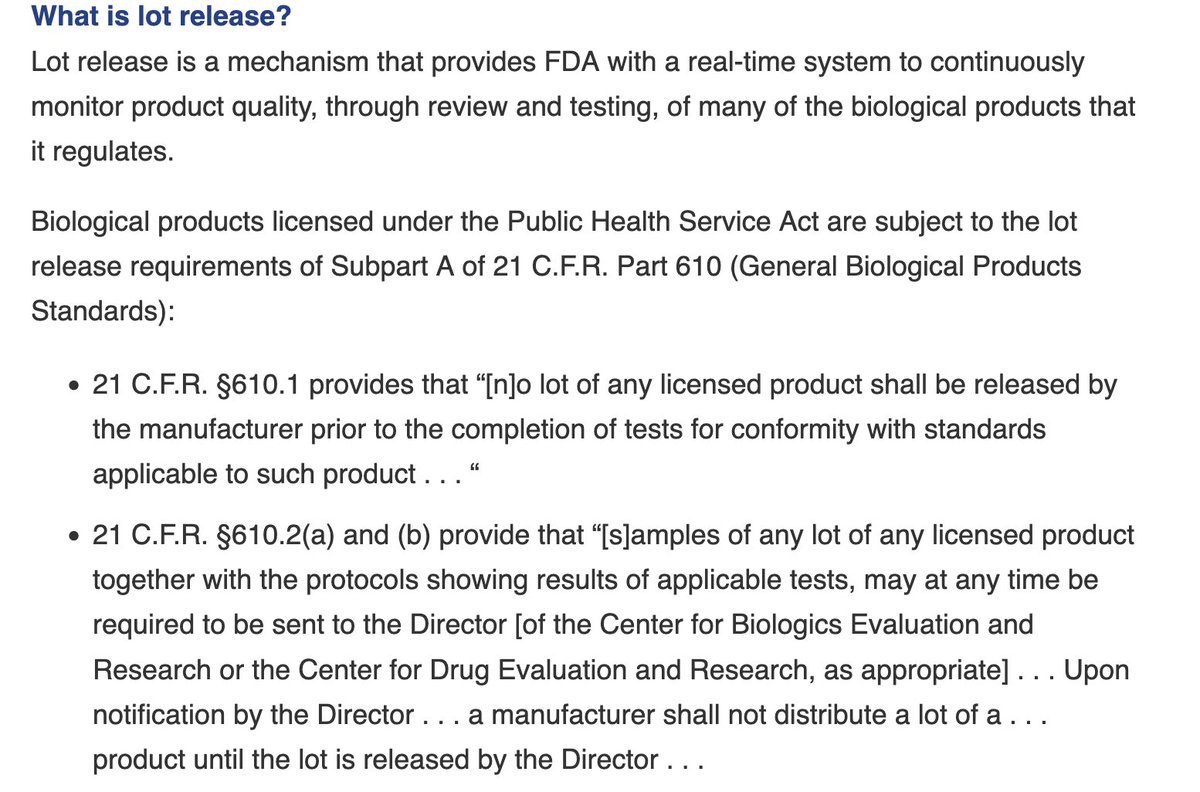
For each batch manufactured, the FDA still performs lot release. This is a quality assurance step.
This process can add an estimated 2-4 days of delay.
fda.gov/vaccines-blood…
For each batch manufactured, the FDA still performs lot release. This is a quality assurance step.
This process can add an estimated 2-4 days of delay.
fda.gov/vaccines-blood…
By the way, you can have a pharmacy check lot release status by looking up Novavax's NDC (National Drug Code) on their supplier's website (e.g., via the McKesson Connect web interface).
If the lot is "on hold" wait a few days; if it shows “FDA-released,” it can be administered.
If the lot is "on hold" wait a few days; if it shows “FDA-released,” it can be administered.
Long story short, in 2024 pharmacies began scheduling Novavax appointments in early September and administering it mid-September.
Sanofi being in control of distribution is an additional variable this year, but they've got more experience with distribution than Novavax ever had.
Sanofi being in control of distribution is an additional variable this year, but they've got more experience with distribution than Novavax ever had.
• • •
Missing some Tweet in this thread? You can try to
force a refresh























