📰 News coverage of the NMCB research consortium on ME/CFS.
Science editor of De Volkskrant, one of the largest papers in the Netherlands, interviews Jos Bosch consortium project leader.
Some highlights below and a link to the article.
1/
Science editor of De Volkskrant, one of the largest papers in the Netherlands, interviews Jos Bosch consortium project leader.
Some highlights below and a link to the article.
1/
Facts noted about the project:
➡️ All academic hospitals participating
➡️ Over €7m euro gov. funding available
➡️ Large biobank being established
➡️ 6 studies underway
➡️ Expansion thereof is planned
2/
➡️ All academic hospitals participating
➡️ Over €7m euro gov. funding available
➡️ Large biobank being established
➡️ 6 studies underway
➡️ Expansion thereof is planned
2/
Background to the consortium:
➡️ Began in 2013 via citizen's initiative
➡️ ME patients gathered petition w/ 50k signatures
➡️ Which led to advisory opinion from Health Council
➡️ ... which finally recommended investing in biomedical research
3/
➡️ Began in 2013 via citizen's initiative
➡️ ME patients gathered petition w/ 50k signatures
➡️ Which led to advisory opinion from Health Council
➡️ ... which finally recommended investing in biomedical research
3/
Patients sit on the board and the research program and approach are based on their input.
"It's incredible how much knowledge patients possess," says Bosch."
4/
"It's incredible how much knowledge patients possess," says Bosch."
4/
"His workplace at the Amsterdam UMC is just around the corner from the post-COVID expertise center that opened there at the end of last year. This is for good reason: doctors and scientists collaborate."
5/
5/
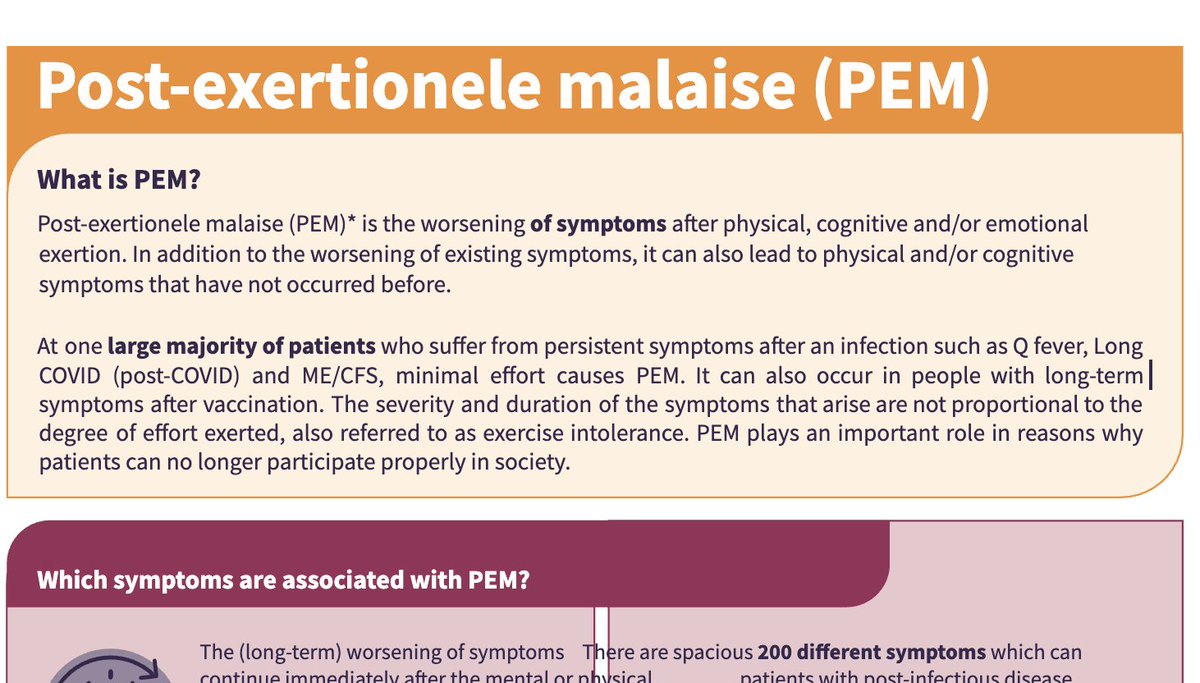
"The clinical features overlap; many post-COVID patients have symptoms of ME/CFS. The aftermath of an infection is something many patients share; for the majority of ME/CFS patients, symptoms began after an infection."
6/
6/
"Patients with chronic Q fever (contracted by a bacterium in goats or sheep) and chronic Lyme disease (contracted after a tick bite) have similar symptoms. Therefore, in addition to post-COVID, these two post-infectious diseases are also included in the study."
7/
7/
"A biobank is being developed with bodily material from two thousand people: patients from four groups and, as a control, a group of healthy individuals."
"They will complete questionnaires and perform tests."
8/
"They will complete questionnaires and perform tests."
8/
"[Researchers] don't have to spend a large portion of their time and budget recruiting patients first. And, importantly, there's funding for eight years. This allows us to retain researchers for a longer period."
9/
9/
"Q: If the disease isn't taken seriously, were researchers even available?
For the 1st rnd of consultations, we'd sent invitations to hospitals and universities, we'd rented a room, and I expected at most a handful of interested parties. To my surprise, the room was full."
10/
For the 1st rnd of consultations, we'd sent invitations to hospitals and universities, we'd rented a room, and I expected at most a handful of interested parties. To my surprise, the room was full."
10/
"Many doctors offered same explanation: because of the success of medicine, they're increasingly seeing serious illnesses become chronic. And these patients sometimes have the same symptoms as patients with ME. Patients with MS or RA, for example, can also experience intense exhaustion or unexplained pain."
11/
11/
"Doctors are no longer surprised by it. Some even told me: I think we've always mistreated patients with chronic fatigue syndrome."
12/
12/
"Q: You said the patients are in charge. Did they have any special requests?
A: At their request, children and young people are also participating in the study, which is unique worldwide. Another special feature: they wanted us to include homebound patients. In international studies, at most a few percent of patients are bedridden. Yet, we can learn the most from this group. That's why we'll soon be visiting patients at home."
13/13
A: At their request, children and young people are also participating in the study, which is unique worldwide. Another special feature: they wanted us to include homebound patients. In international studies, at most a few percent of patients are bedridden. Yet, we can learn the most from this group. That's why we'll soon be visiting patients at home."
13/13
Article: archive.md/hfidp
• • •
Missing some Tweet in this thread? You can try to
force a refresh