🧵”The AMA strongly supports the Department of Health and Human Services’ @HHSGov recent decision to upgrade #Medicare Plan Finder so patients can choose plans that actually include their trusted physicians and hospitals.” 

2/ “This…mirrors AMA’s January 2025 advocacy calling for HHS to integrate plan network data into Plan Finder. Once this is complete, patients no longer will be forced to click through multiple websites just to confirm if their physicians are in-network.
tinyurl.com/5869nja2
tinyurl.com/5869nja2

3/ Patients can compare plans:
Medicare Advantage (Part C)
Medicare Prescription Drug (Part D)
Medigap plans at :
After entering zip code, meds, preferred pharmacies, the tool generates a list of plans available in the area, along with estimated costs.medicare.gov
Medicare Advantage (Part C)
Medicare Prescription Drug (Part D)
Medigap plans at :
After entering zip code, meds, preferred pharmacies, the tool generates a list of plans available in the area, along with estimated costs.medicare.gov
4/📍AMA has:
• heard from patients struggling to navigate Plan Finder
• urged HHS to deliver a 1-stop tool where patients can:
-verify if a doctor or hospital is in network
-filter plans by specialty, location, language, hospital affiliation
-avoid post-enrollment surprises
• heard from patients struggling to navigate Plan Finder
• urged HHS to deliver a 1-stop tool where patients can:
-verify if a doctor or hospital is in network
-filter plans by specialty, location, language, hospital affiliation
-avoid post-enrollment surprises
5/📍AMA urges steps to ensure Plan Finder is user-friendly:
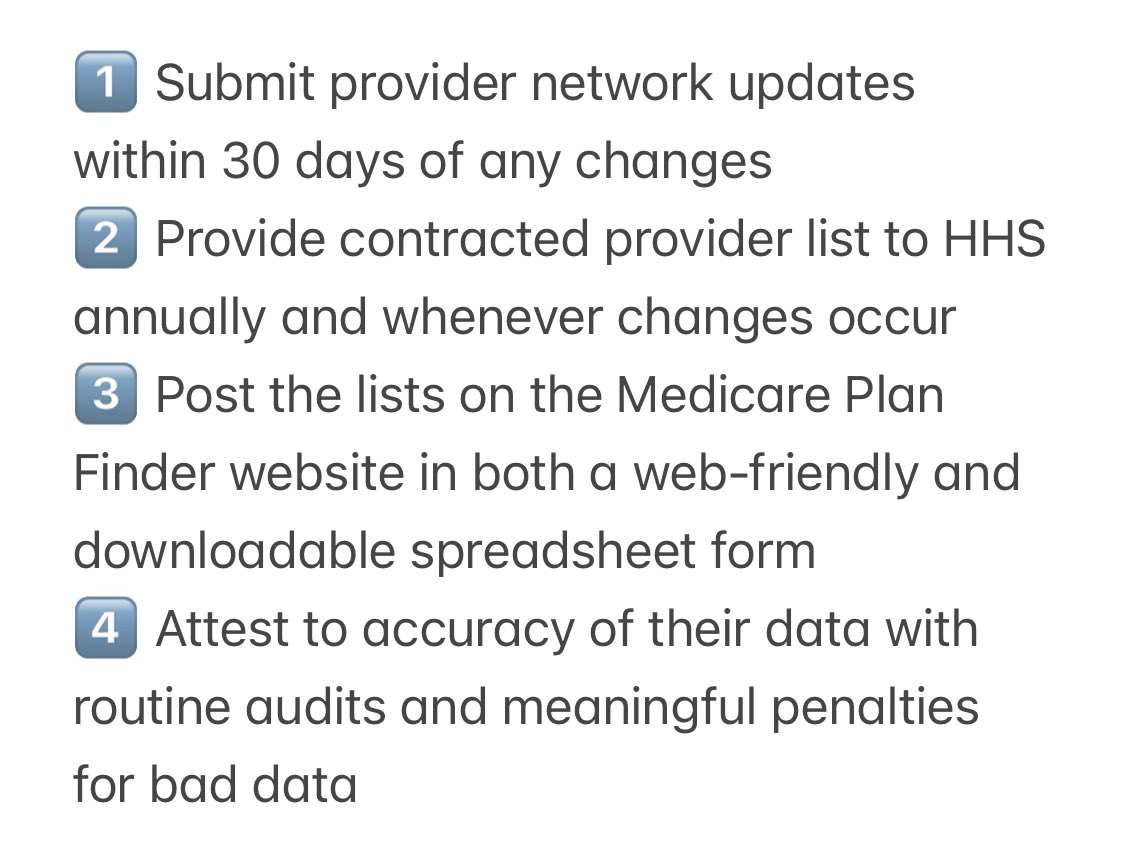
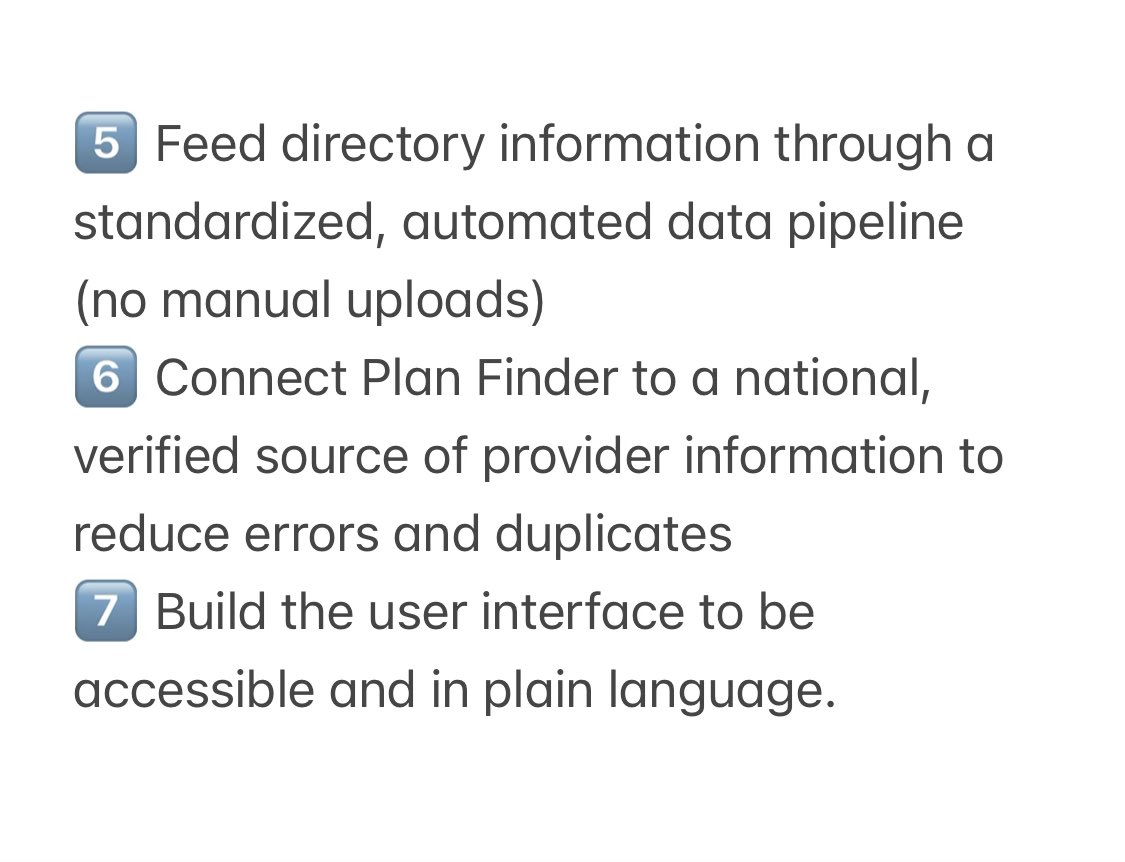
To ensure the upgraded Plan Finder is accurate and reliable, the AMA urges HHS to require Medicare Advantage plans to take these 7 steps ⤵️
To ensure the upgraded Plan Finder is accurate and reliable, the AMA urges HHS to require Medicare Advantage plans to take these 7 steps ⤵️
6/ @PresAmerMed said:
“We commend HHS’ intent and commitments—and see this as a clear response to persistent @AmerMedicalAssn advocacy on behalf of physicians and our patients.”
Also ⤵️
“We commend HHS’ intent and commitments—and see this as a clear response to persistent @AmerMedicalAssn advocacy on behalf of physicians and our patients.”
Also ⤵️
• • •
Missing some Tweet in this thread? You can try to
force a refresh