Some encouraging news for THR science! 🎉
A deeply flawed article on e-cigarettes & cancer has just been retracted, following a letter to the editor criticizing the paper. 👇
@RetractionWatch
Original article: doi.org/10.1016/j.jcpo…
A deeply flawed article on e-cigarettes & cancer has just been retracted, following a letter to the editor criticizing the paper. 👇
@RetractionWatch
Original article: doi.org/10.1016/j.jcpo…
2) The original article was a systematic review which concluded:
"E-cigarette use may be associated with an increased risk of certain cancers, including cervical and breast cancer. However, the evidence remains inconclusive, and more rigorous longitudinal studies are needed"
"E-cigarette use may be associated with an increased risk of certain cancers, including cervical and breast cancer. However, the evidence remains inconclusive, and more rigorous longitudinal studies are needed"
3) However, as Miguel & Steffensen (who consult to RAI) pointed out in a letter to the editor, there were many severe flaws:
1⃣ There were large (and undisclosed) deviations from the preregistered protocol for the search:
(Below is my summary, not from the article)
1⃣ There were large (and undisclosed) deviations from the preregistered protocol for the search:
(Below is my summary, not from the article)
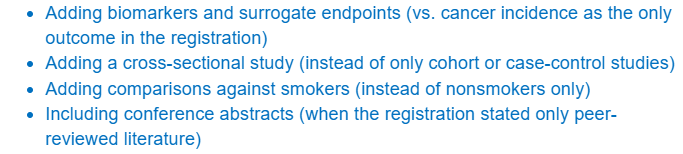
4) 2⃣ The stated search criteria was supposed to capture nonsmokers only... (a good idea to avoid confounding by smoking history)
... but the paper includes comparisons with smokers, which means the search criteria were changed and/or not described properly.
... but the paper includes comparisons with smokers, which means the search criteria were changed and/or not described properly.
5) 3⃣ The original article mis-categorized studies it reviewed, claiming that biomarker or inflammatory studies were "case-control studies" of cancer incidence:

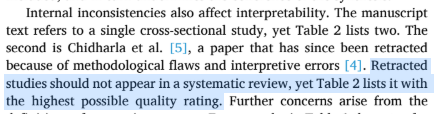
6) It's also not clear whether there is n=1 or n=2 cross-sectional studies in the review.
This is inconsistent in different parts of the paper. One of these studies is a retracted paper:
This is inconsistent in different parts of the paper. One of these studies is a retracted paper:
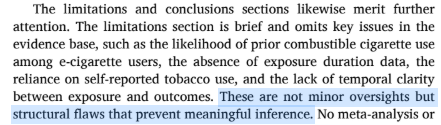
7) 4⃣ The original article omits key limitations of the review and the underlying primary studies:
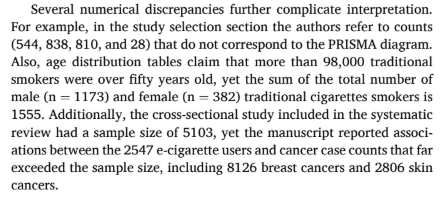
8) 5⃣ Finally, there were glaring inconsistencies in even the most basic numbers reported:
9) The editor-in-chief's retraction note echoes all of these major flaws.
This was not raised in the criticism or retraction note, but given the weird numeric mismatches, I have to wonder if parts of the original review were AI-generated.
Kudos to all involved! 🙌
This was not raised in the criticism or retraction note, but given the weird numeric mismatches, I have to wonder if parts of the original review were AI-generated.
Kudos to all involved! 🙌
• • •
Missing some Tweet in this thread? You can try to
force a refresh