Spinal injections 💉 strongly NOT recommended for chronic back, neck and sacroliliac pain ⛔️
Here's a 🧵 on the recent (and controversial) BMJ study and why I think some caution is needed here.
Here's a 🧵 on the recent (and controversial) BMJ study and why I think some caution is needed here.
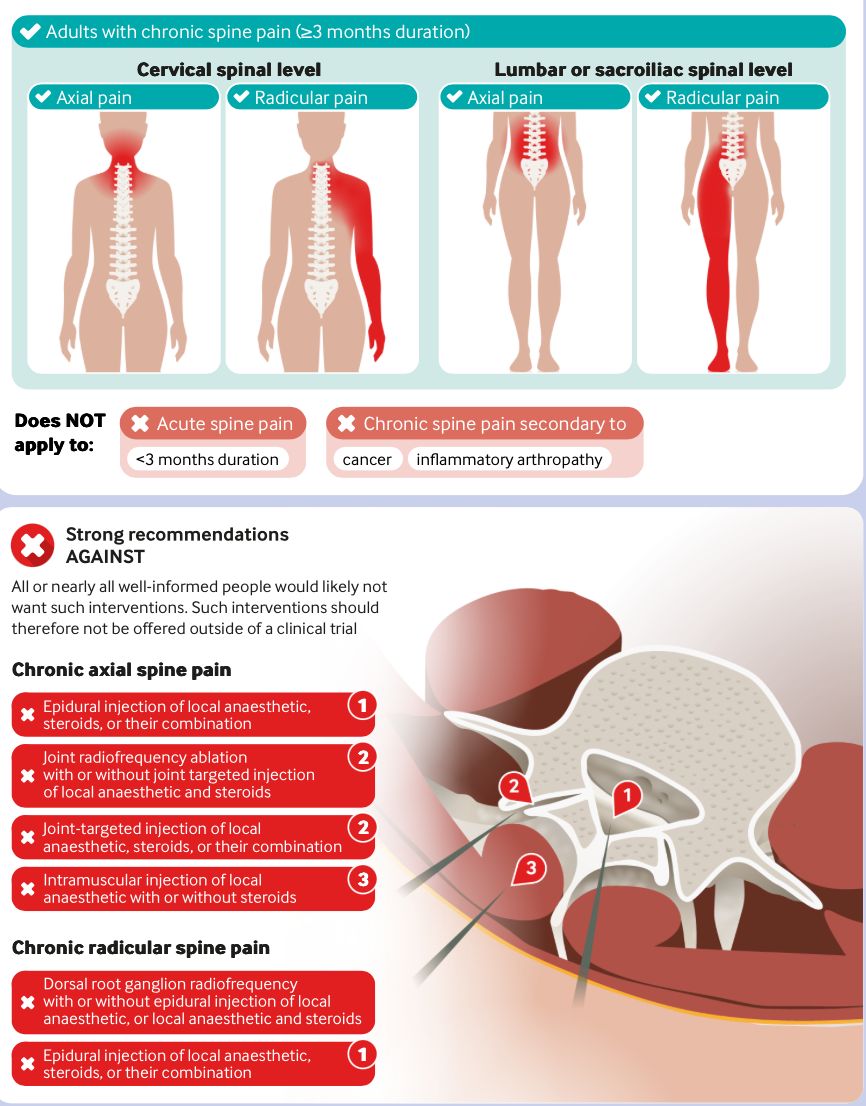
This guideline looked at chronic (≥3 months) non-cancer spine pain.
Based on a large systematic review + network meta-analysis.
Investigated efficacy of:
• Epidural steroid injections
• Facet joint injections
• Radiofrequency ablation
• Intramuscular injections
Based on a large systematic review + network meta-analysis.
Investigated efficacy of:
• Epidural steroid injections
• Facet joint injections
• Radiofrequency ablation
• Intramuscular injections

The key finding:
👉 Strong recommendations AGAINST injections
WHY?
Because benefits are:
• Small
• Often clinically trivial
• Short-lived
Other issues include
• Cost
• Burden
• Procedural risks (infection, dural puncture, neuro complications etc )
Even if rare—they matter at scale.
👉 Strong recommendations AGAINST injections
WHY?
Because benefits are:
• Small
• Often clinically trivial
• Short-lived
Other issues include
• Cost
• Burden
• Procedural risks (infection, dural puncture, neuro complications etc )
Even if rare—they matter at scale.
I understand this research and why the recommendations were made but cant fully endorse the findings for 3️⃣main reasons....
1️⃣ Because many patients (in my experience) still get meaningful benefit from injections post >3 months after onset of pain.
This pain reduction (although temporary) can be a very helpful to provide a window to perform rehab, improve patients physical condition and help them to move towards self-efficacy.
This pain reduction (although temporary) can be a very helpful to provide a window to perform rehab, improve patients physical condition and help them to move towards self-efficacy.
2️⃣ By the time many patients seek care and are then referred to pain services it is normally > 3 months.
In our service from the time of referral to the pain team is >1 year.
Should we exclude these patients from pain care altogether?
In our service from the time of referral to the pain team is >1 year.
Should we exclude these patients from pain care altogether?
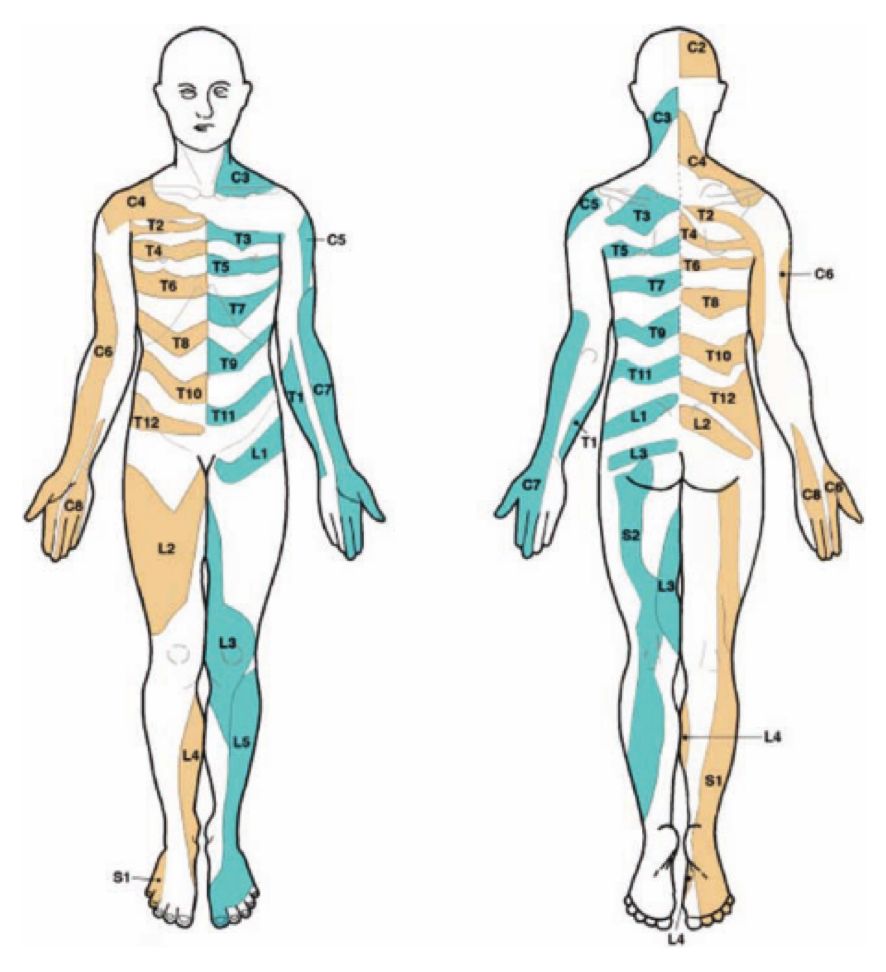
3️⃣ Radicular symptoms can easily last 6-12 months after onset. Should we deny people extra pain relief over this time if conservative measures and oral analgesia are implemented but minimally effective (and surgery is not a strong option)?
🙋♂️Ask any sciatica patient if they would like 8-12 weeks of reduced pain.....the answer would be unanimous I reckon....
🙋♂️Ask any sciatica patient if they would like 8-12 weeks of reduced pain.....the answer would be unanimous I reckon....
Final Thoughts 💭
• There are undoubtedly patients who are having repeated, ineffectual injections out there and we definitely want to see less of this.
• But should this come at the expense of denying relief to a certain number of patients who actually need it?
• In a condition like radiculopathy which can be very recalcitrant and where treatment options are not plentiful, taking one therapeutic agent off the table so soon (>3months) seems too stringent in my book.
👉Making blanket rejections seem heavy-handed to me.
👉 I favor a balanced approach guided by individual patient needs - not hard time cutoffs.
• There are undoubtedly patients who are having repeated, ineffectual injections out there and we definitely want to see less of this.
• But should this come at the expense of denying relief to a certain number of patients who actually need it?
• In a condition like radiculopathy which can be very recalcitrant and where treatment options are not plentiful, taking one therapeutic agent off the table so soon (>3months) seems too stringent in my book.
👉Making blanket rejections seem heavy-handed to me.
👉 I favor a balanced approach guided by individual patient needs - not hard time cutoffs.
That's just my opinion.
What are your thoughts?
What are your thoughts?
@neilorpen
@Retlouping
@DerekGriffin86
@k8purcellphysio
@AdamStenman
@adamdobson123
@marklaslett_NZ
@CorKinetic
@northwoods1980
@Retlouping
@DerekGriffin86
@k8purcellphysio
@AdamStenman
@adamdobson123
@marklaslett_NZ
@CorKinetic
@northwoods1980
@cormac_mullins would love your take on this
• • •
Missing some Tweet in this thread? You can try to
force a refresh