It is pretty unprecedented for WHO to declare a PHEIC so rapidly after detecting an outbreak, but it is absolutely merited in this case.
This is a scary one.
Why?
- Very late detection
- Difficult context
- Limited countermeasures
- and global response tools got DOGE-d
🧵...
This is a scary one.
Why?
- Very late detection
- Difficult context
- Limited countermeasures
- and global response tools got DOGE-d
🧵...
https://twitter.com/DrTedros/status/2055879914620964932
It's instructive to compare this against other major past outbreaks.
The largest Ebola outbreak in history, West Africa/2014 (which I worked on for @USAID), was detected at a far earlier stage (49 cases / 29 deaths) than this one (246 cases/65 deaths).
Deaths are now >88 and ⬆️
The largest Ebola outbreak in history, West Africa/2014 (which I worked on for @USAID), was detected at a far earlier stage (49 cases / 29 deaths) than this one (246 cases/65 deaths).
Deaths are now >88 and ⬆️
This one has already built up more momentum at time of detection.
Worrying because Ebola risk and response scale in an exponential, not linear, fashion.
Each extra uncontrolled case means tens of more people potentially exposed in super spreading events.
Worrying because Ebola risk and response scale in an exponential, not linear, fashion.
Each extra uncontrolled case means tens of more people potentially exposed in super spreading events.
That in turn requires tens more response staff per additional case to treat patients, run lab samples, trace and monitor contacts, etc.
I wrote about the huge difficulties of scaling up Ebola response in 2014 in this paper:
cgdev.org/publication/st…
I wrote about the huge difficulties of scaling up Ebola response in 2014 in this paper:
cgdev.org/publication/st…

Second point of comparison: location.
DRC has a lot of experience with Ebola and tends to control outbreaks quickly when they are in govt-controlled areas.
EXCEPT the last outbreak in the East, which got massively out of control, killed 2300, and required a huge int'l response.
DRC has a lot of experience with Ebola and tends to control outbreaks quickly when they are in govt-controlled areas.
EXCEPT the last outbreak in the East, which got massively out of control, killed 2300, and required a huge int'l response.
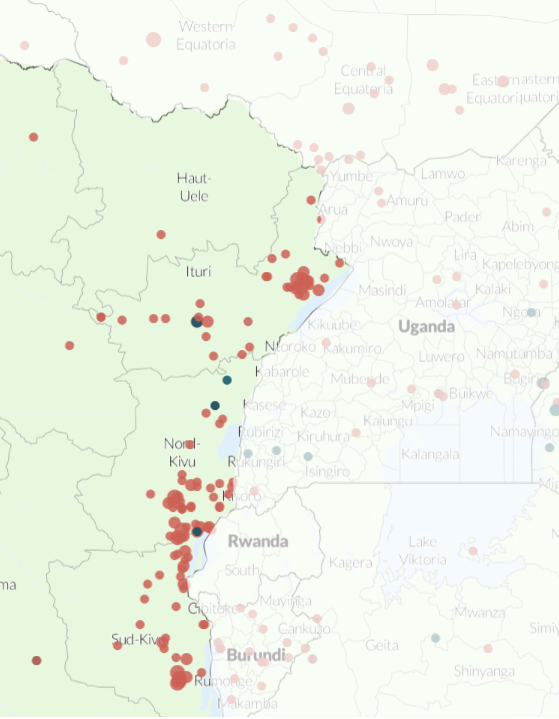
Eastern DRC is a very tough place to mount a major outbreak response. There is active conflict in Ituri and much of the region. These are incidents of violence in the past month:
acleddata.com/update/africa-…
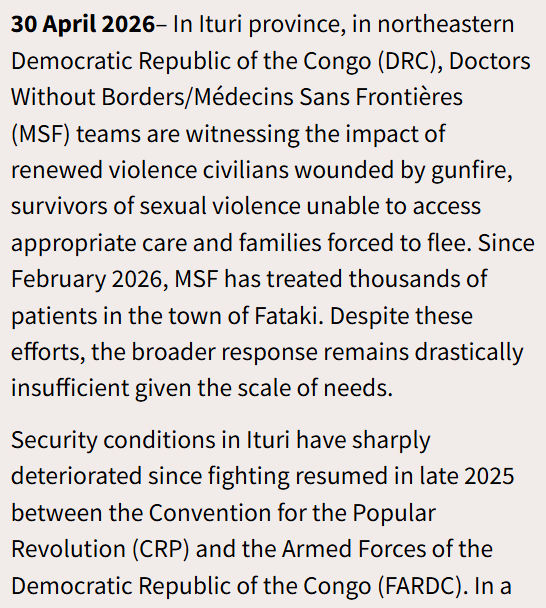
And reporting from MSF on rising violence recently: msfsouthasia.org/drc-new-wave-o…
acleddata.com/update/africa-…
And reporting from MSF on rising violence recently: msfsouthasia.org/drc-new-wave-o…
Notably, the huge outbreak in E. DRC in 2018-19 was the Ebola-Zaire strain, which has a highly effective vaccine and other medical countermeasure developed during the 2014-15 W. Africa outbreak.
That brings us to the third comparison - this is a different strain with no vaccine.
That brings us to the third comparison - this is a different strain with no vaccine.
So if a vaccine-preventable strain of Ebola in the same region could generate over 2300 deaths, this one could very well be worse.
Controlling it will require a major global response to support the DRC Ministry of Health.
Um...about that....
Controlling it will require a major global response to support the DRC Ministry of Health.
Um...about that....
Fourth point of comparison with past responses:
Most of the international infrastructure that we relied on in past outbreaks...has been DOGE-d.
In 2014, USAID and CDC, supported by the US military, led the international response.
USAID is gone and CDC is decimated.
Most of the international infrastructure that we relied on in past outbreaks...has been DOGE-d.
In 2014, USAID and CDC, supported by the US military, led the international response.
USAID is gone and CDC is decimated.
USAID had a dedicated outbreak response division that tackled Ebola and other outbreaks.
@elonmusk fired that team in the midst of a small Ebola outbreak in Uganda last year, then lied about it.
Today that team, like USAID, no longer exists.
npr.org/sections/goats…
@elonmusk fired that team in the midst of a small Ebola outbreak in Uganda last year, then lied about it.
Today that team, like USAID, no longer exists.
npr.org/sections/goats…
In E. DRC/2018, the USG response was smaller but @WHO made one of the largest deployments in its history to help DRC get the outbreak under control.
WHO at least still exists! But it is currently reeling from huge budget cuts after Trump withdrew and cut off all US funding.
WHO at least still exists! But it is currently reeling from huge budget cuts after Trump withdrew and cut off all US funding.
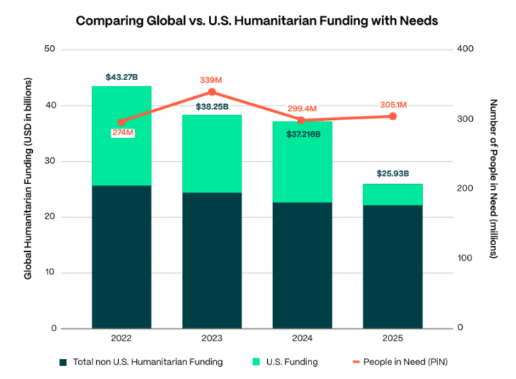
WHO's funding for health emergencies has dropped by 37% since 2024, and it has been forced to lay off thousands of staff around the world. Meanwhile its emergency contingency fund is close to empty.
Tough starting point to mount a major response.
apps.who.int/gb/ebwha/pdf_f…
Tough starting point to mount a major response.
apps.who.int/gb/ebwha/pdf_f…
So the landscape for international support is pretty...yikes.
Which is frustrating because Ebola (unlike early COVID) is a virus that we understand pretty well by now, and for which we have solid blueprints for large scale response...IF the money and expertise are deployed.
Which is frustrating because Ebola (unlike early COVID) is a virus that we understand pretty well by now, and for which we have solid blueprints for large scale response...IF the money and expertise are deployed.
So, what needs to happen now?
Move FAST to activate financing and deploy surge capacity to support DRC MoH.
Ebola response only gets more intensive and expensive the longer you wait to ramp it up. Pinching pennies now will mean higher bills later.
Move FAST to activate financing and deploy surge capacity to support DRC MoH.
Ebola response only gets more intensive and expensive the longer you wait to ramp it up. Pinching pennies now will mean higher bills later.
And the US needs to get in the game.
The dismantling of US-funded health programming in DRC by DOGE is likely a big factor in why this outbreak was detected so late.
Important not to compound that mistake with a slow and tepid USG response now.
The dismantling of US-funded health programming in DRC by DOGE is likely a big factor in why this outbreak was detected so late.
Important not to compound that mistake with a slow and tepid USG response now.
CDC has – or at least had – a lot of vital expertise. The administration needs deploy those folks; remove the stupid, performative restrictions on contact between CDC and WHO; and just let them engage in a fully unfettered way to contain this outbreak.
USAID is gone, but a handful of experienced Ebola responders shifted over to State.
This would be a good time to activate them onto a DART for Congo, and ramp up the funding, as the first Trump administration did in 2018 when USAID still existed.
This would be a good time to activate them onto a DART for Congo, and ramp up the funding, as the first Trump administration did in 2018 when USAID still existed.
This is an all-hands-on-deck situation. Other donors will have to step up, whether or not the US does. The post-DOGE USG, with an RFK-led health dept, will be erratic at best.
Clock is ticking - time to act. This will get exponentially harder the longer things wait.
//end
Clock is ticking - time to act. This will get exponentially harder the longer things wait.
//end
• • •
Missing some Tweet in this thread? You can try to
force a refresh