NEW: @jessesingal with new revelations, based on FOIAs, about the Johanna Olson-Kennedy-led, @NIH-funded ($10m) research initiative on pediatric gender medicine. 🧵
NIH was misled with help from @wpath and @TheEndoSociety.
NIH was misled with help from @wpath and @TheEndoSociety.

Olson-Kennedy and her colleagues intended to study the effects of puberty blockers and cross-sex hormones in minors.
NIH initially "expressed qualms" about the proposed study being observational rather experimental. Singal explains the difference, and why it matters.
NIH initially "expressed qualms" about the proposed study being observational rather experimental. Singal explains the difference, and why it matters.
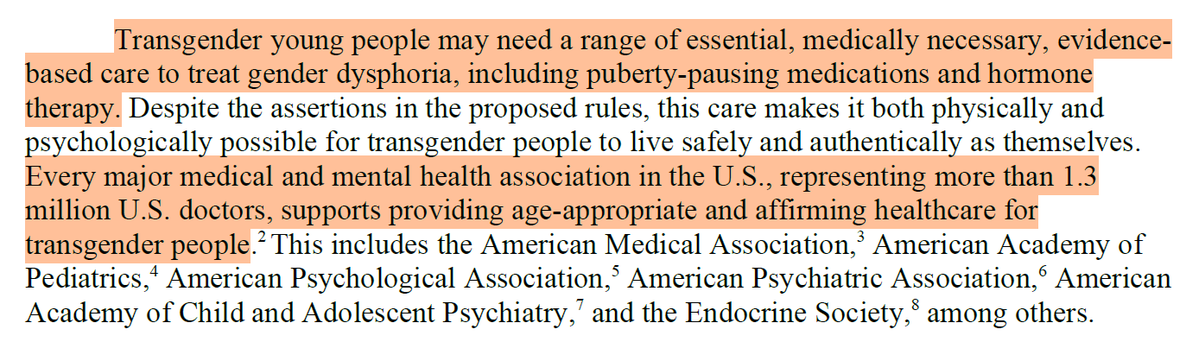
With support from @wpath and @TheEndoSociety, however, Olson-Kennedy told NIH that the treatments are known to work and that withholding them (i.e., having a control group) would be unethical.
The researchers received letters of support for their NIH application from @wpath and @TheEndoSociety.
Singal obtained those letters and copies are linked in the piece.
Singal obtained those letters and copies are linked in the piece.
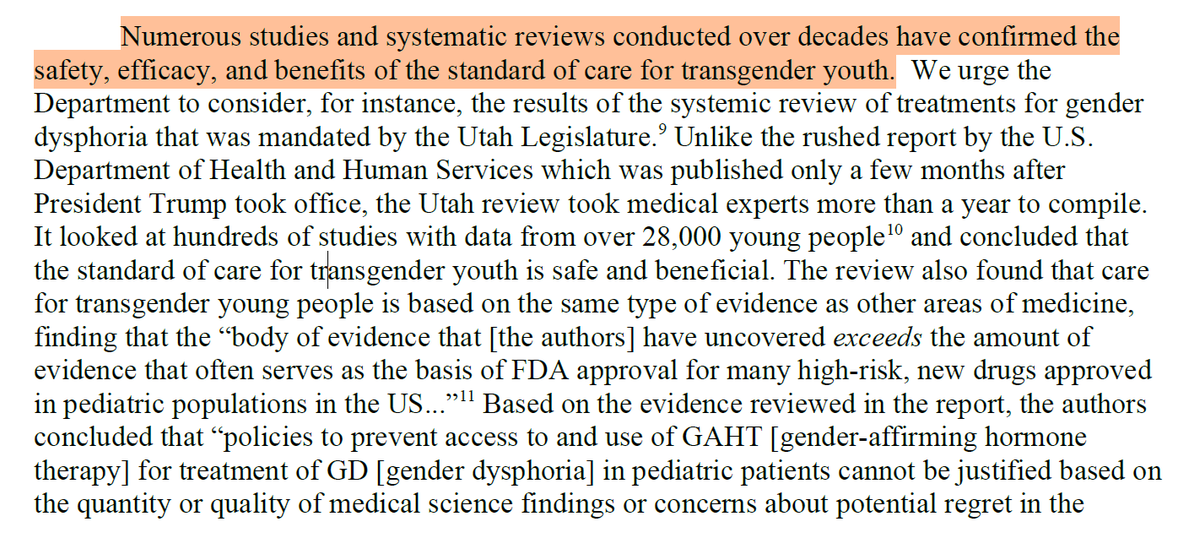
But the claim about effectiveness (and by extension, the unethical nature of an experiment) was unsupported by evidence.
And crucially, Olson-Kennedy and her colleagues themselves knew it was not true, at least not about the patient cohort they intended to study.
And crucially, Olson-Kennedy and her colleagues themselves knew it was not true, at least not about the patient cohort they intended to study.
Olson-Kennedy's application to the NIH therefore contained an obvious contradiction. They insisted that puberty blockers and cross-sex hormones are known to be effective, but also that they need NIH (taxpayer) money to study whether they are effective.
Rather than note the contradiction and act on its significance, NIH granted the funding.
For discussion of these revelations and more, read Singal's piece here:
jessesingal.substack.com/p/how-wpath-an…
For discussion of these revelations and more, read Singal's piece here:
jessesingal.substack.com/p/how-wpath-an…
• • •
Missing some Tweet in this thread? You can try to
force a refresh