
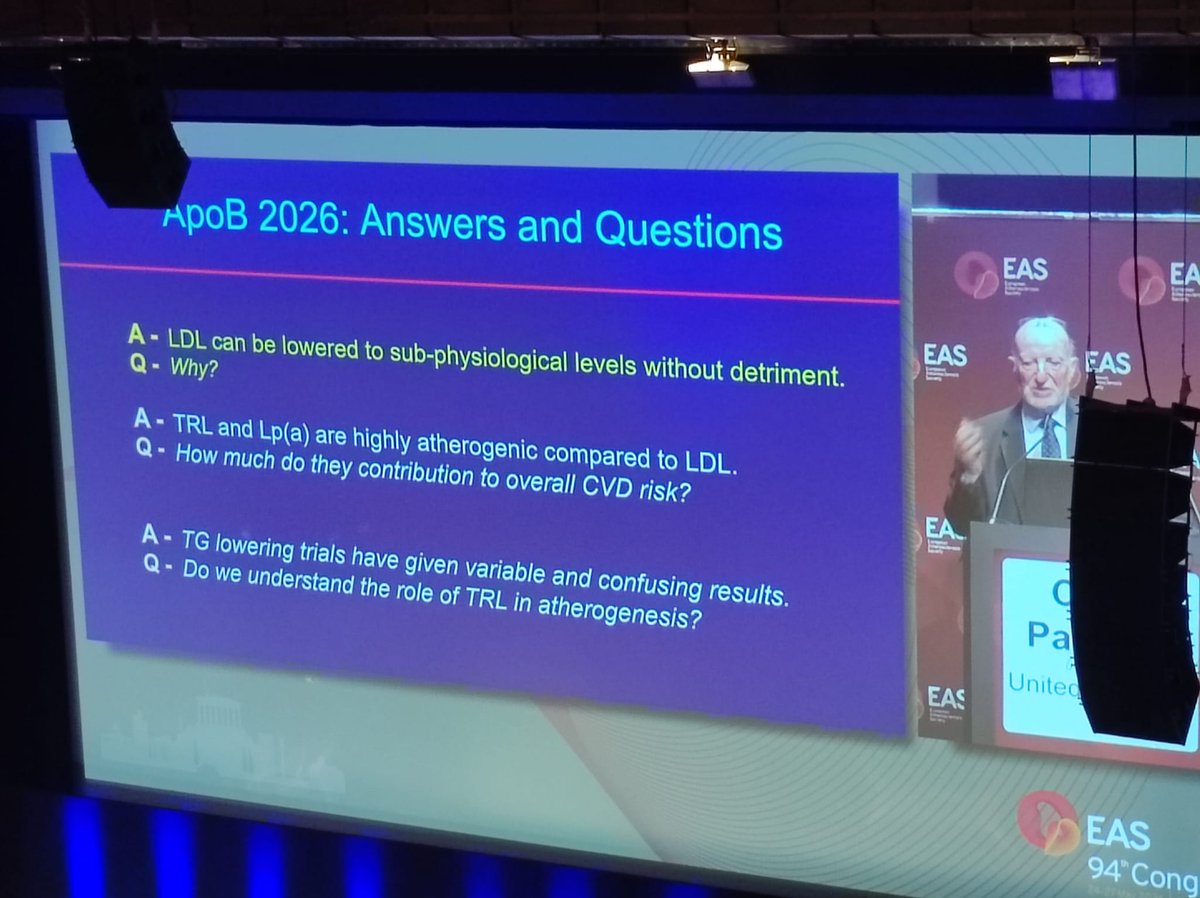
ApoB in 2026: the question is no longer whether ApoB matters. The question is how far ApoB can take us in understanding which particles drive risk (LDL, TRL/remnants, Lp(a)) and how we should act on them. #EASCongress2026 #MyEAS2026 

One key message: LDL-C can be lowered to very low levels without apparent detriment. But ApoB reminds us that risk is not only about cholesterol mass. It is also about the number and biology of atherogenic particles. #EASCongress2026 #MyEAS2026
@society_eas @EASCongress LDL, TRL/remnants and Lp(a) do not contribute equally across patients. ApoB may give us the particle burden, but the next step is understanding the risk-weight of different ApoB-containing particles.
That is where residual risk becomes more interesting.
#EASCongress2026
That is where residual risk becomes more interesting.
#EASCongress2026

@society_eas @EASCongress TRL/remnant particles may be fewer than LDL particles, but they may carry disproportionate risk.
Genetics suggests TRL/remnant cholesterol can be highly atherogenic, possibly reflecting cholesterol content, inflammation, or both. #EASCongress2026 #MyEAS2026
Genetics suggests TRL/remnant cholesterol can be highly atherogenic, possibly reflecting cholesterol content, inflammation, or both. #EASCongress2026 #MyEAS2026

@society_eas @EASCongress TG-lowering trials have taught us humility. Some positive. Some neutral. Some confusing. Maybe the real question is not simply “do triglycerides matter?” but which TRL biology, which patient phenotype, and which therapeutic target matter most. #EASCongress2026 #MyEAS2026

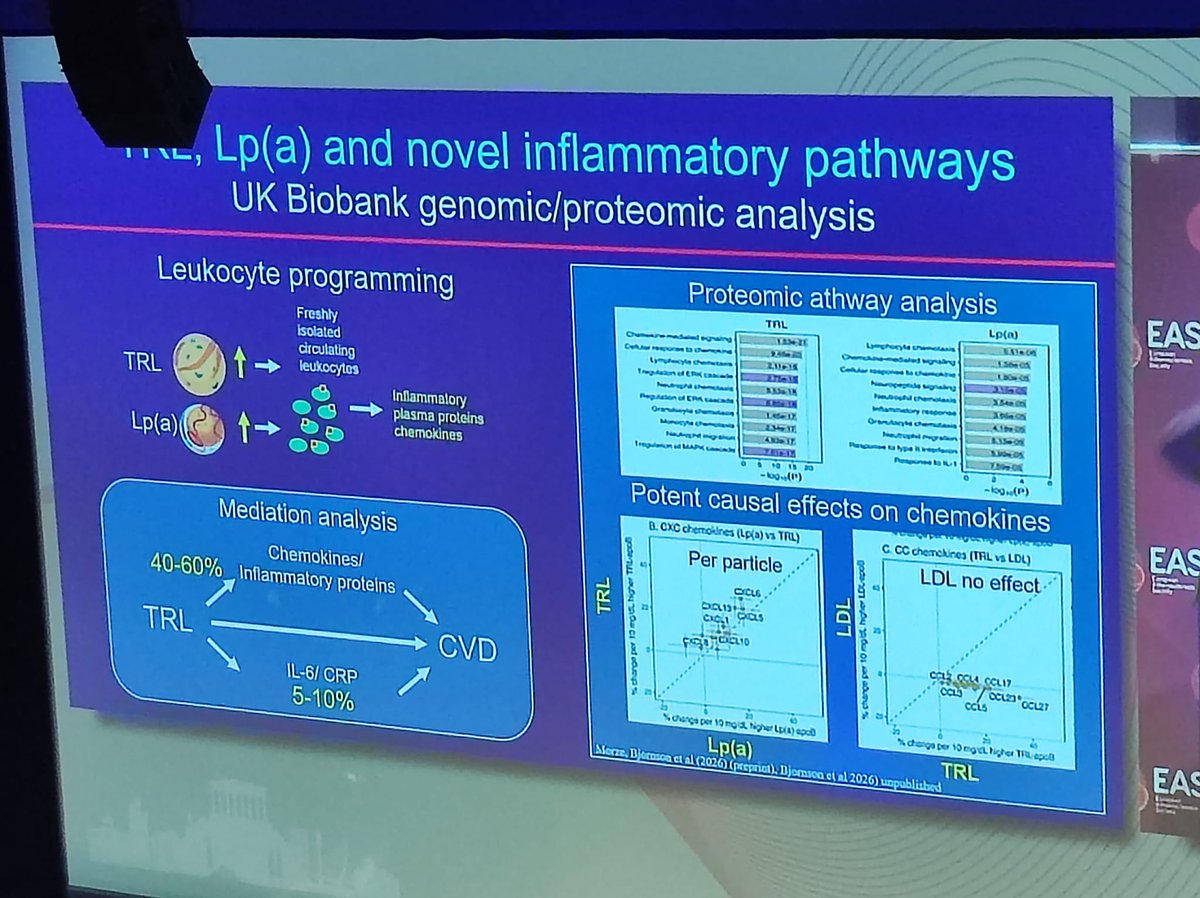
@society_eas @EASCongress A particularly intriguing point: TRL and Lp(a) may not be only lipid particles. They may also interact with leukocyte programming, chemokines and inflammatory pathways. Residual lipid risk and residual inflammatory risk may be closer than we think. #EASCongress2026 #MyEAS2026
@society_eas @EASCongress Take-home from this keynote: ApoB is becoming more than a “better LDL marker”. It is a framework to integrate particle number, particle type, atherogenicity and biology.
ApoB 2026 is not only answers. It is better questions.
#EASCongress2026 #MyEAS2026
ApoB 2026 is not only answers. It is better questions.
#EASCongress2026 #MyEAS2026

• • •
Missing some Tweet in this thread? You can try to
force a refresh



