
📢Japan has just posted meeting materials for their annual COVID strain selection, and there’s some good news, but also, by my estimation, some potentially very bad news…
Here is the presentation from Takeda, which is Novavax’s partner in Japan who completes strain selection duties and manufacturers the Nuvaxovid antigen: mhlw.go.jp/content/109060…
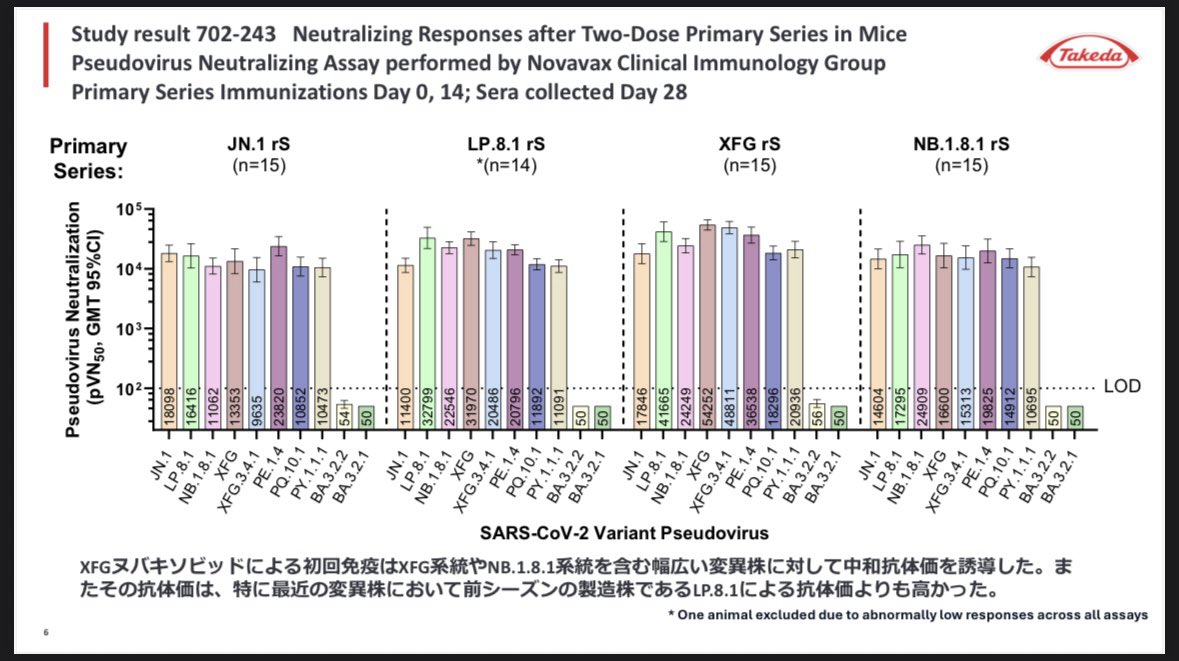
In the first slide, they directly compare a priming series of JN.1, LP.8.1, XFG, and NB.1.8.1. The result is very clearly that XFG provides the best response across the entire JN.1 lineage, so it’s a good thing that the FDA and Sanofi have chosen XFG as the 2026-2027 variant. Notably, however, there is almost no neutralization at all against BA.3.2 variants.
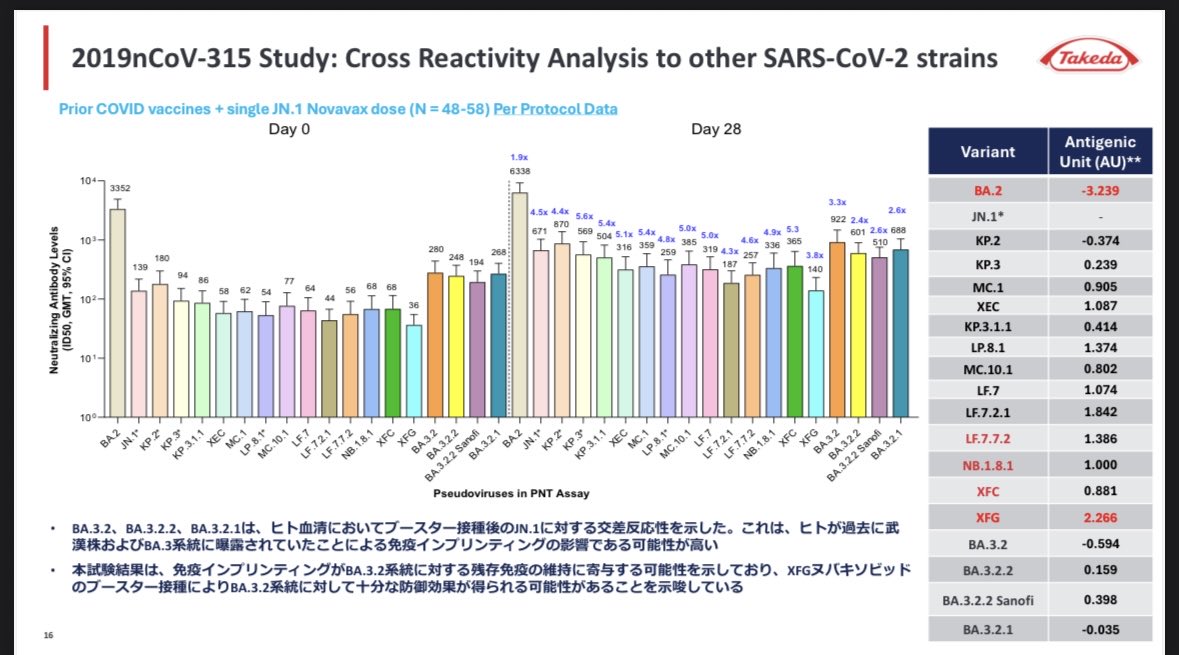
On the next slide, they’re showing that the JN.1 vaccine actually has really good cross-reactivity to BA.3.2 variants. The weakest cross-reactivity is against the XFG variant, so once again, this shows that it’s the best choice for the 2026-2027 update.
When it comes to the conflicting BA.3.2 results, my takeaway is that current JN.1/XFG vaccines can expand antibody coverage against it pretty well, but that is entirely reliant upon having imprinting against early SARS2 variants (which someone would’ve gotten either through exposure or vaccination). Well, if someone has never had COVID before, and they’ve also never gotten an ancestral mRNA vaccine (which causes stronger imprinting), then that may put that person at a significant disadvantage when it comes to protection against BA.3.2. That includes myself…and I’m guessing many of my followers as well.
There’s not much that we can do about that, except to hope that multiple doses of Nuvaxovud keep doing their thing to expand antibody coverage across a wide range of variants. This is part of why I always stress the importance of completing a new 3-dose series within a year when someone is switching to Nuvaxovid for the first time - it’s not a “one and done” type deal if you want to get the best results. And it’s also why folks should consider dosing every 6 months, instead of only once annually. Nothing is guaranteed either way, but that will gives it a much better chance of expanding the antibody range to cover BA.3.2 in a meaningful way.
Here is a link to the full meeting materials: mhlw.go.jp/stf/shingi2/ne…
Here is the presentation from Takeda, which is Novavax’s partner in Japan who completes strain selection duties and manufacturers the Nuvaxovid antigen: mhlw.go.jp/content/109060…
In the first slide, they directly compare a priming series of JN.1, LP.8.1, XFG, and NB.1.8.1. The result is very clearly that XFG provides the best response across the entire JN.1 lineage, so it’s a good thing that the FDA and Sanofi have chosen XFG as the 2026-2027 variant. Notably, however, there is almost no neutralization at all against BA.3.2 variants.
On the next slide, they’re showing that the JN.1 vaccine actually has really good cross-reactivity to BA.3.2 variants. The weakest cross-reactivity is against the XFG variant, so once again, this shows that it’s the best choice for the 2026-2027 update.
When it comes to the conflicting BA.3.2 results, my takeaway is that current JN.1/XFG vaccines can expand antibody coverage against it pretty well, but that is entirely reliant upon having imprinting against early SARS2 variants (which someone would’ve gotten either through exposure or vaccination). Well, if someone has never had COVID before, and they’ve also never gotten an ancestral mRNA vaccine (which causes stronger imprinting), then that may put that person at a significant disadvantage when it comes to protection against BA.3.2. That includes myself…and I’m guessing many of my followers as well.
There’s not much that we can do about that, except to hope that multiple doses of Nuvaxovud keep doing their thing to expand antibody coverage across a wide range of variants. This is part of why I always stress the importance of completing a new 3-dose series within a year when someone is switching to Nuvaxovid for the first time - it’s not a “one and done” type deal if you want to get the best results. And it’s also why folks should consider dosing every 6 months, instead of only once annually. Nothing is guaranteed either way, but that will gives it a much better chance of expanding the antibody range to cover BA.3.2 in a meaningful way.
Here is a link to the full meeting materials: mhlw.go.jp/stf/shingi2/ne…
By the way, and for whatever it’s worth:
Sanofi’s data presented at the FDA meeting last week does essentially show this same thing, with these 2 slides, but in a *much* more convoluted way. I wouldn’t have pieced two and two together here without the Takeda slides
Sanofi’s data presented at the FDA meeting last week does essentially show this same thing, with these 2 slides, but in a *much* more convoluted way. I wouldn’t have pieced two and two together here without the Takeda slides


• • •
Missing some Tweet in this thread? You can try to
force a refresh




