
#IDgrandrounds 50/M with new HIV diagnosis (CD4 13), presents with miliary TB and pericarditis (moderate pericardial effusion, no evidence of constrictive physiology). Together with anti-TB medications, will you prescribe corticosteroids?
1/5) No strong evidence to support the use of steroids especially in people w/ HIV.
Guidelines differ however:
ATS/CDC/IDSA 2016 idsociety.org/practice-guide…:
-- initial steroids "not be routinely used"
WHO 2017 who.int/tb/publication…:
-- initial steroids "maybe used"
Guidelines differ however:
ATS/CDC/IDSA 2016 idsociety.org/practice-guide…:
-- initial steroids "not be routinely used"
WHO 2017 who.int/tb/publication…:
-- initial steroids "maybe used"
2/5) A recent meta-analysis (from our very own Dr. Ige George), showed no mortality difference w/ the use of steroids (Forest plot provided in the pic)
ingentaconnect.com/content/iuatld…
ingentaconnect.com/content/iuatld…
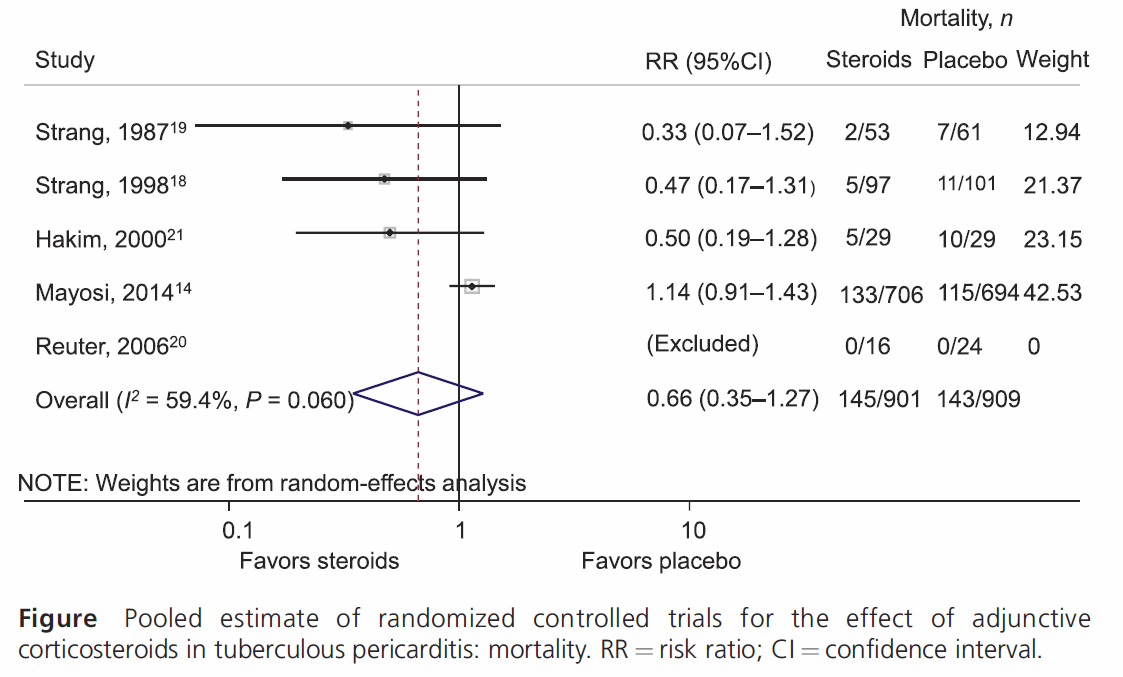
3/5) Largely driven by the largest RCT (Mayosi): nejm.org/doi/10.1056/NE…
-- 67% HIV (14% on ART)
-- no mortality benefit
-- reduction in constrictive pericarditis
WHO guideline: HIV in the Mayosi trial may have influenced result; people w/o HIV may still benefit from steroids.
-- 67% HIV (14% on ART)
-- no mortality benefit
-- reduction in constrictive pericarditis
WHO guideline: HIV in the Mayosi trial may have influenced result; people w/o HIV may still benefit from steroids.
4/5) In the same meta-analysis by George et al ingentaconnect.com/content/iuatld…
.. a sensitivity analysis was performed to assess the impact of hypothetical NEW studies to the meta-analysis (see Forest plot in the pic).
The results were the same.
.. a sensitivity analysis was performed to assess the impact of hypothetical NEW studies to the meta-analysis (see Forest plot in the pic).
The results were the same.

5/5) On the side..
The great Sir William Osler was believed to have suffered from cutaneous TB (tuberculosis verrucosa cutis or prosecrutor's wart). Through out his career, he had performed >1,000 postmortem autopsies.
Read more here: sciencedirect.com/science/articl…
The great Sir William Osler was believed to have suffered from cutaneous TB (tuberculosis verrucosa cutis or prosecrutor's wart). Through out his career, he had performed >1,000 postmortem autopsies.
Read more here: sciencedirect.com/science/articl…

• • •
Missing some Tweet in this thread? You can try to
force a refresh




