#WCLC19 @rdoebele kicks off the plenary with a discussion of tumor agnostic therapy. Really refers to biology driven. Our current siloed approach to oncology is a bit of a barrier to this strategy. Timing favored lung cancer as the field where this became mainstream. #OncoAlert 


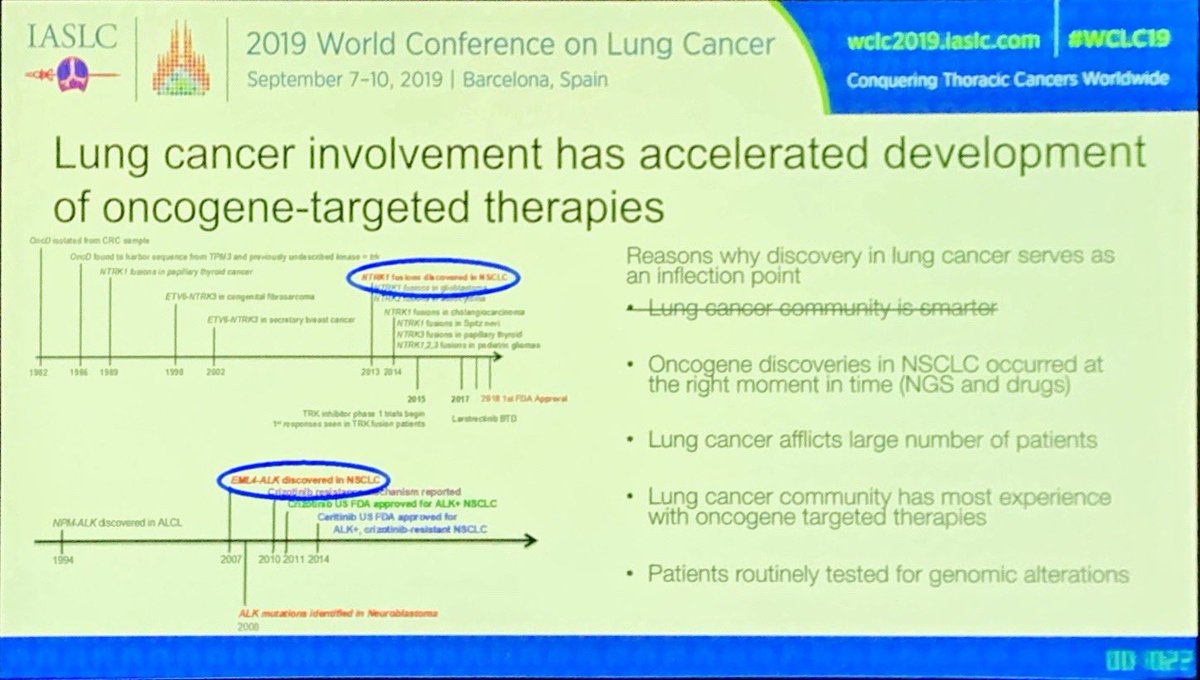
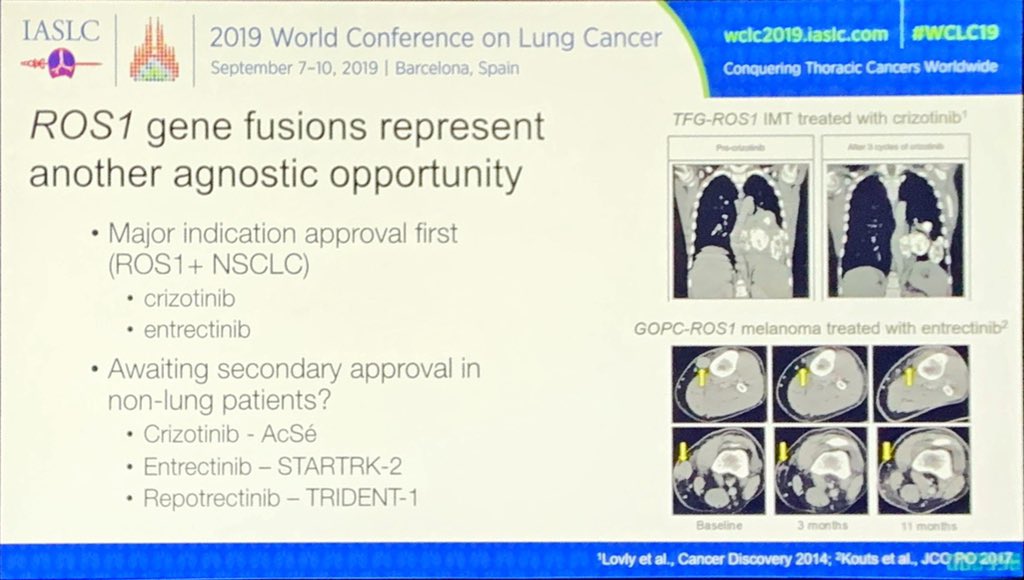
#NTRK is a great example where we see efficacy across tumors and no indication of a specific tumor type resistant to inhibition. But we see similar themes in #ALK and #ROS1 - will there be a regulatory path forward? #OncoAlert #WCLC19

Importantly, resistance also seems to be tumor agnostic. Similar mutations seen mediating resistance across tumor types. Predicting #NRG1 as next important target across tumor types. Biology is more dependent on the genomics than the histology! #WCLC19 #OncoAlert


• • •
Missing some Tweet in this thread? You can try to
force a refresh