#ESMO19 Taking some time to cross pollinate by attending some non-lung sessions. Melanoma increasingly relevant for all of oncology. Also helps that the speaker is friend and @LombardiCancer colleague (and boss) Mike Atkins, my go-to expert for any immunotherapy question! 


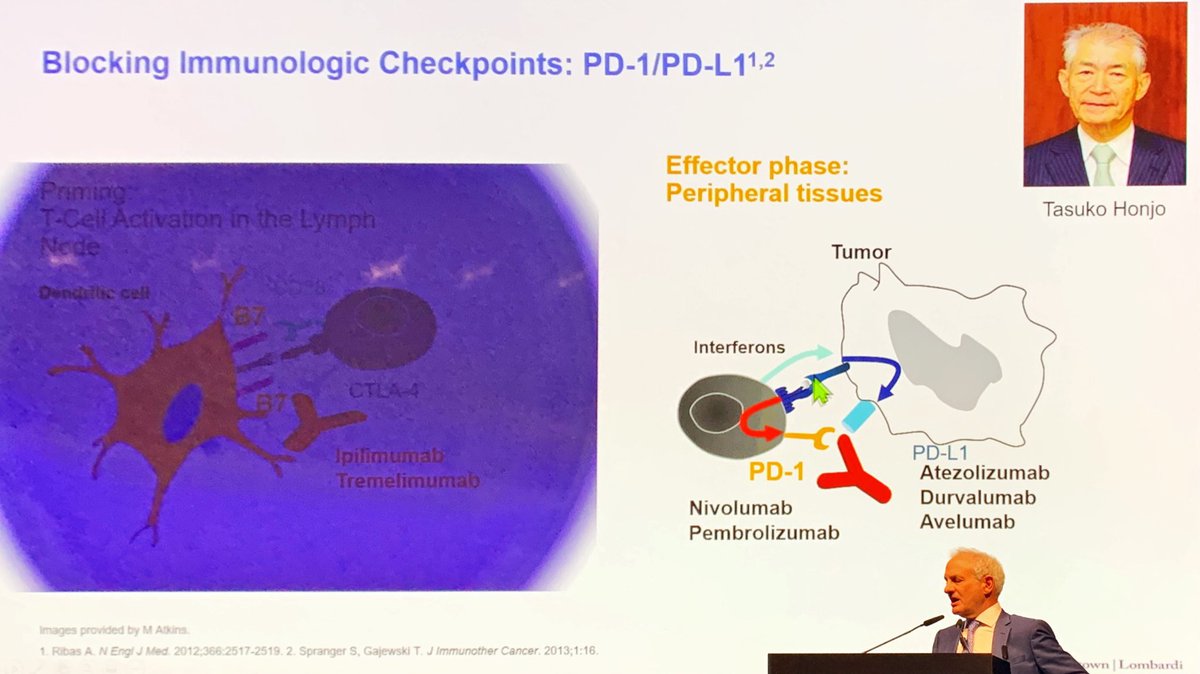
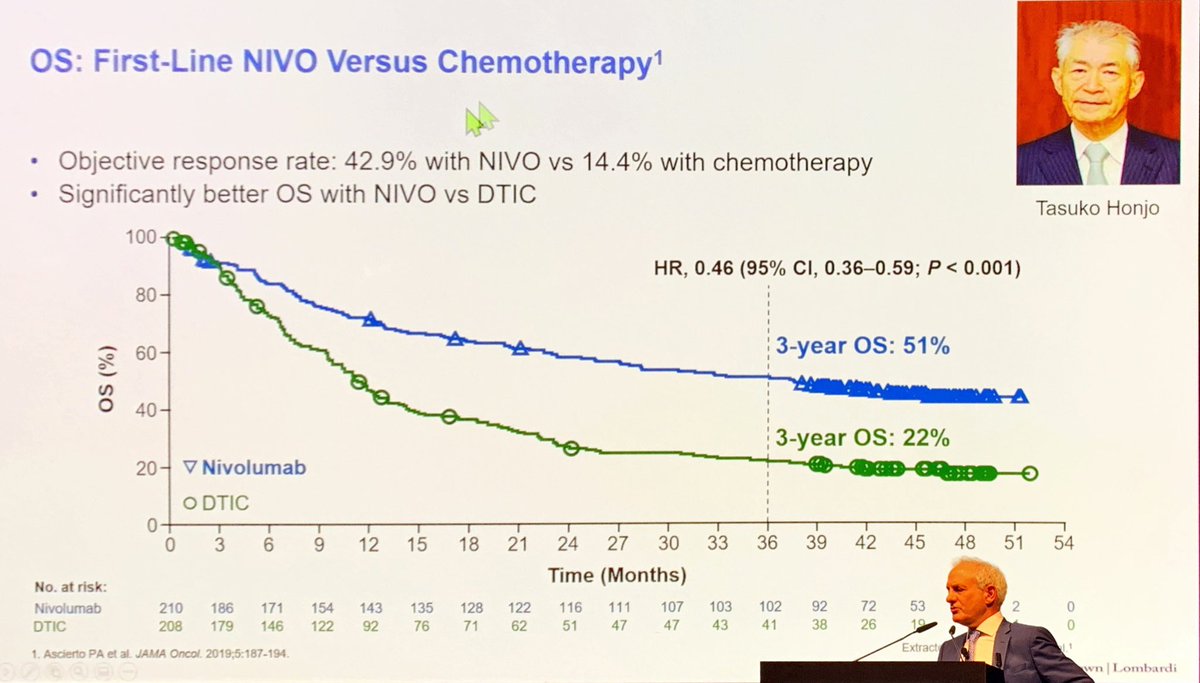
#ESMO19 Mike Atkins with throwbacks to IL-2 and the key advances of Allison and Honjo. Nivo beats chemo in melanoma and changes the field forever. We owe our progress throughout oncology to these early landmark studies. Curative therapy with long follow up.

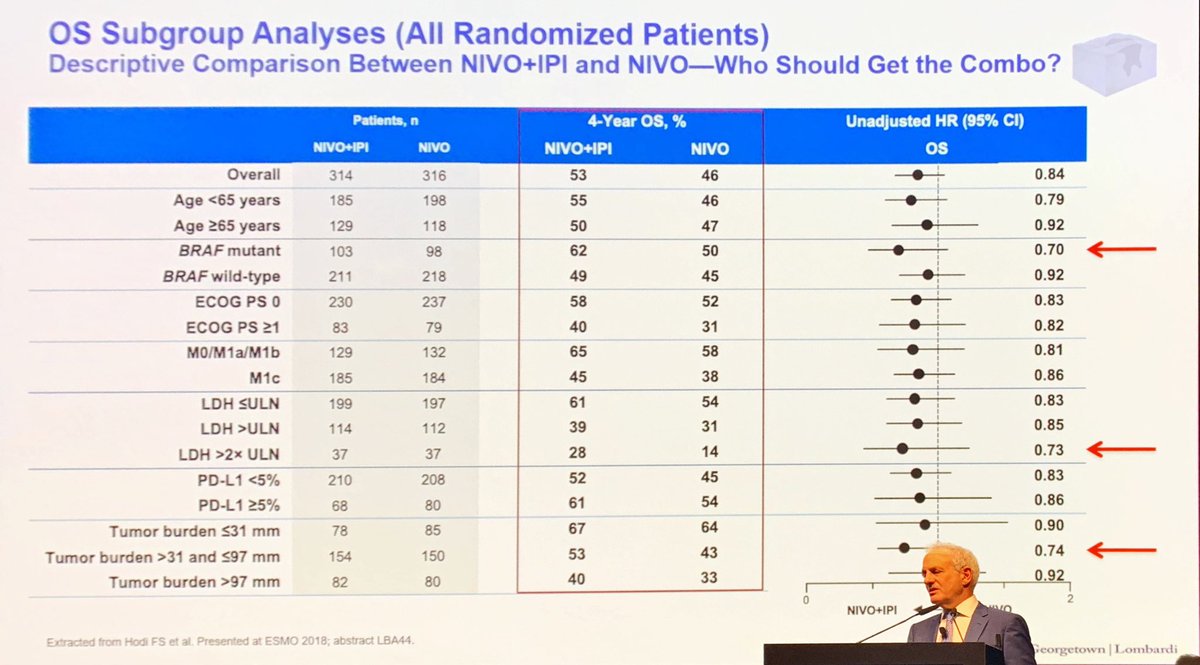
#ESMO19 found this interesting. Who specifically benefits from CTLA4? In nivo/ipi vs nivo, groups that did better with addition of ipi were BRAF+, high LDH, high tumor burden (not mutational burden - disease burden). Parallels in lung cancer?
• • •
Missing some Tweet in this thread? You can try to
force a refresh