RV resuscitation! screen for RV failure with POCUS (and records if you have em) #thepeoplesventricle #StoweEM20 by @mattroginski 


incorrect probe rotation can cause RV size to be underestimated! Matt’s own echo has great TAPSE #humblebrag #StoweEM20 by @mattroginski


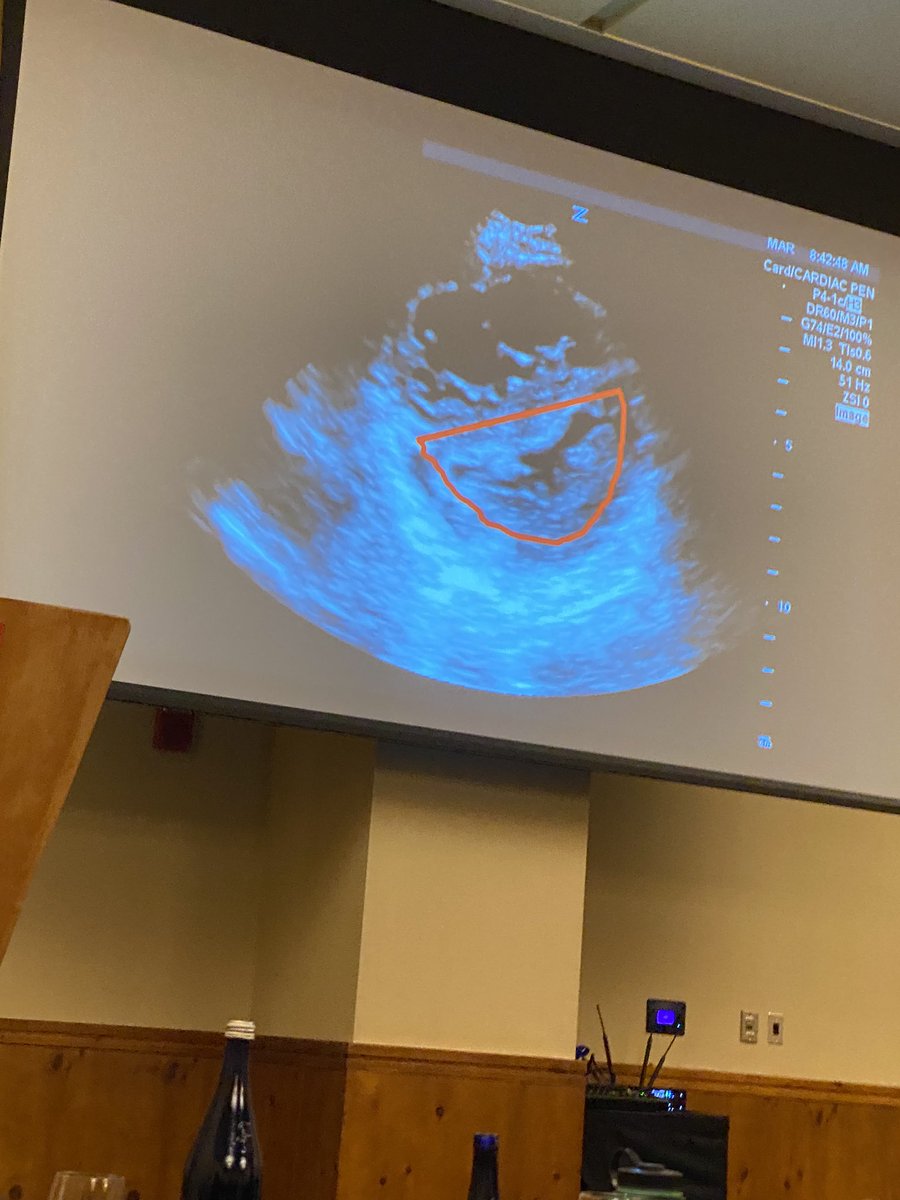

signs of severe badness: with bubble injection:
- bubbles take forever to clear (CO is aweful, blood isnt going anywhere)
- right to left shunt
#StoweEM20 by @mattroginski
- bubbles take forever to clear (CO is aweful, blood isnt going anywhere)
- right to left shunt
#StoweEM20 by @mattroginski

- juditious volume management
- early pressor
- arrhythmia tx
- avoid intubation if possible
#StoweEM20 by @mattroginski
- early pressor
- arrhythmia tx
- avoid intubation if possible
#StoweEM20 by @mattroginski




• • •
Missing some Tweet in this thread? You can try to
force a refresh