
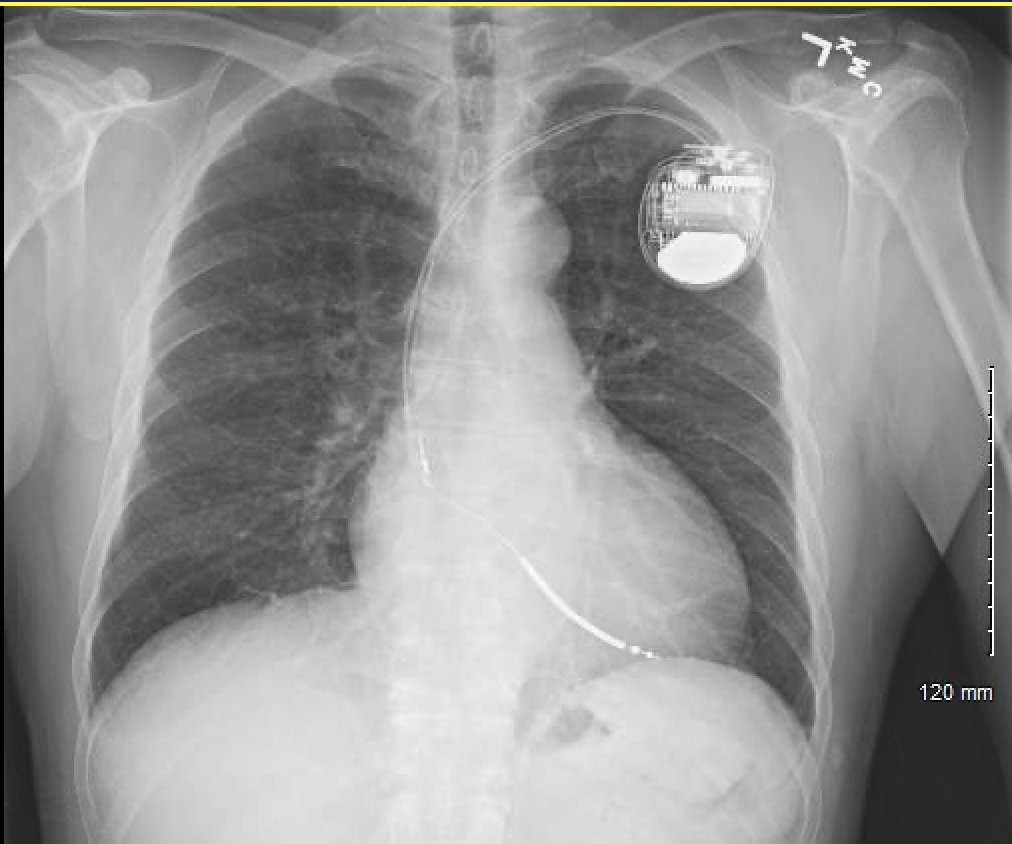

My concern — agree w others. Feared ICD lead crossed PFO into LV. This was next day CXR after new implant.
Action— echo
Findings — Lead in RV. All OK. Pt discharged home.
@sgreenbergmd @DrGregMichaud @dlschermd @SchakrabartiEP @badinmd @MarkStephanMD @DrDeese99 @J_RyanJordan
Action— echo
Findings — Lead in RV. All OK. Pt discharged home.
@sgreenbergmd @DrGregMichaud @dlschermd @SchakrabartiEP @badinmd @MarkStephanMD @DrDeese99 @J_RyanJordan
@sgreenbergmd @DrGregMichaud @dlschermd @SchakrabartiEP @badinmd @MarkStephanMD @DrDeese99 @J_RyanJordan Let’s talk about issue of LV lead placement.
In placing lead, helps to have disciplined routine.
First confirm you are in vein. Sounds easy, but in very sick pt with expected high venous pressure you can be fooled. Happened to me once. Never again, I hope.
In placing lead, helps to have disciplined routine.
First confirm you are in vein. Sounds easy, but in very sick pt with expected high venous pressure you can be fooled. Happened to me once. Never again, I hope.
@sgreenbergmd @DrGregMichaud @dlschermd @SchakrabartiEP @badinmd @MarkStephanMD @DrDeese99 @J_RyanJordan Best way to confirm without doubt you in vein, next arterial or extra cardiac is to advance wire into IVC. If you can go below diaphragm, you are good. Not always easy, but if any doubt go to that effort.
@sgreenbergmd @DrGregMichaud @dlschermd @SchakrabartiEP @badinmd @MarkStephanMD @DrDeese99 @J_RyanJordan OK, you are sure you are in the vein, that doesn’t mean you can’t get over to the left ventricle. Leads can cross PFO or ASD. You also wanna stay out of the middle cardiac vein.
Best way to confirm you are in RV is by carefully watching lead passage with disciplined routine.
Best way to confirm you are in RV is by carefully watching lead passage with disciplined routine.
When you get lead into RA, put your flouro in RAO. Harder to get fooled in RAO. The RV will be splayed out to the R side of the screen.
Shape a big pigtail curve on your stylet and pass the lead through TV (prolapse is best) and get it all the way up past PV like a SG catheter.
Shape a big pigtail curve on your stylet and pass the lead through TV (prolapse is best) and get it all the way up past PV like a SG catheter.
If you can get this position in the PA, like a SG catheter, you know you aren’t in the MCV or left atrium
Exchange for straight or gently curved stylet & ease lead back. Watch it drop into RV apex or septum.
Check paced configuration. RBBB is OK. Negative lead I is not OK.
Exchange for straight or gently curved stylet & ease lead back. Watch it drop into RV apex or septum.
Check paced configuration. RBBB is OK. Negative lead I is not OK.
If the lead didn’t drop easily when you withdraw from PA, you might be tangled in the TV apparatus. If any doubt, withdraw all the way back to RA and try again. Maybe make more effort to prolapse this time. If you prolapse, you know you got through TV w/o incident.
If any doubt at this point, pull the fluoro into steep LAO. Make certain you are septal on not on lateral wall. It’s not too easy w/o true lateral to be certain, though.
Next day, look at CXR. If your goal was RV apex, the lead should be anterior on lateral film. If it is hugging the sternum, that’s great. If, like my case it’s midline, maybe some concern. If it’s posterior, that’s bad.
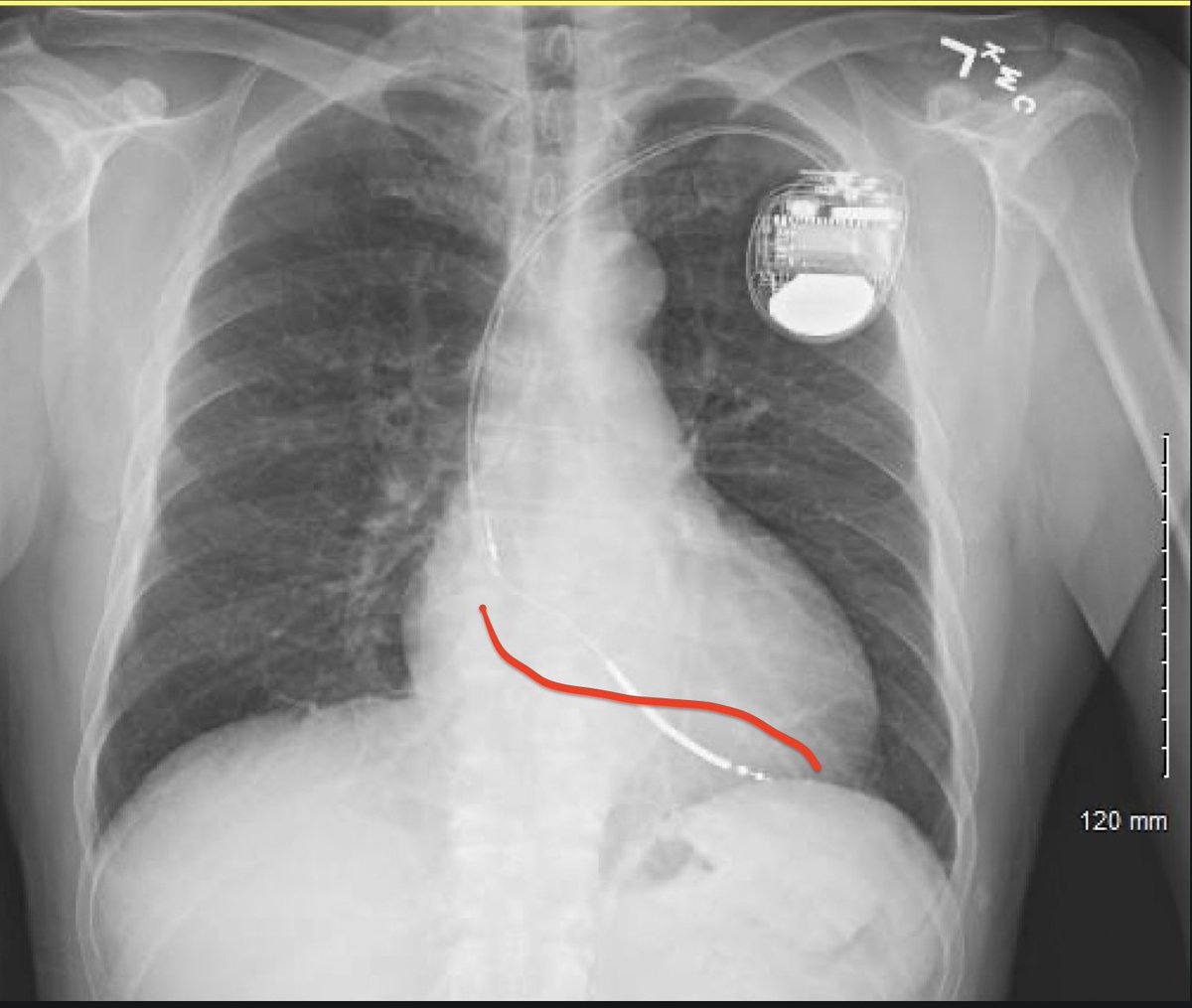
Also look in AP at the crossing point and contour at the TV. If it’s high up, like mine, maybe consider this is the PFO. In the image, I’ve drawn about where I’d have expected the TV crossing to be. Obviously, there is a lot of latitude here, and this lead was ultimately fine. 
So, then, you are making rounds Saturday AM and see this CXR. What to do?
I did the implant. I was pretty darn sure I’d done all these careful steps. Even so, you gotta be certain. Is there any uncertainty? Sure.
We ordered the echo and all was well. Phew.
/fin.
I did the implant. I was pretty darn sure I’d done all these careful steps. Even so, you gotta be certain. Is there any uncertainty? Sure.
We ordered the echo and all was well. Phew.
/fin.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



