Experiment: Surface Best COVID19 threads from @ThreadReaderApp

When is an "aid project" not actually an aid project?
Well, recruiting staff through an anti-Islam biker gang is usually a pretty clear tell.
Beyond the outright insanity of this, it also reveals something important about the agenda behind the GHF. 🧵
Well, recruiting staff through an anti-Islam biker gang is usually a pretty clear tell.
Beyond the outright insanity of this, it also reveals something important about the agenda behind the GHF. 🧵
At first blush this story almost seems too outlandish to be real. Full disclosure - I was skeptical when I first hear these rumblings a few months ago.
But BBC brings the receipts. And the receipts are flat-out nuts (this nugget about gang leader Johnny Mulford is priceless).
But BBC brings the receipts. And the receipts are flat-out nuts (this nugget about gang leader Johnny Mulford is priceless).

Who is Mulford, the lead GHF security subcontractor?
He's a biker gang leader who was formerly debarred by the Pentagon for "bribery, larceny, and making false official statements" related to contract kickbacks.
Not who you'd want near an aid project.
jagcnet.army.mil/Sites/Procurem…
He's a biker gang leader who was formerly debarred by the Pentagon for "bribery, larceny, and making false official statements" related to contract kickbacks.
Not who you'd want near an aid project.
jagcnet.army.mil/Sites/Procurem…


On Friday, when most of America wasn't paying attention, heading out for the holidays, Trump signed an Exec Order transferring ALL control over foreign aid from State to OMB.
This will destroy American overseas programs. Here's why (MORE)whitehouse.gov/presidential-a…
This will destroy American overseas programs. Here's why (MORE)whitehouse.gov/presidential-a…
2/US programs for everything from #famine relief & #HIV care to safe pregnancy efforts & building electricity grids have won America friends in the world & saved 100s of millions of lives. They were nested in the State Dept so our diplomats on the ground can oversee them.
MORE
MORE


3/ By moving foreign aid out of State & into OMB, programs for saving starving children, rescuing families from catastrophes, teaching kids to read, stopping epidemics -- ALL of that now falls under the control of Russell Vought.
Who is Vought?
MOREtrumpwhitehouse.archives.gov/people/russell…
Who is Vought?
MOREtrumpwhitehouse.archives.gov/people/russell…

All week the Israeli govt has mounted a major PR push against @theIPCinfo's Gaza famine declaration.
The @IsraelMFA pushback reveals a basic ignorance (perhaps willful?) of how famines work and how the IPC declares them.
Today the IPC responded. Let's take a look. 🧵
The @IsraelMFA pushback reveals a basic ignorance (perhaps willful?) of how famines work and how the IPC declares them.
Today the IPC responded. Let's take a look. 🧵
The GoI has a thin slide deck of bold-font attacks with no links to supporting data.
The IPC reply has 6 pages of explanatory text plus a new table of additional malnutrition analysis (on top of their original 56-page report).
ipcinfo.org/fileadmin/user…
ipcinfo.org/fileadmin/user…
The IPC reply has 6 pages of explanatory text plus a new table of additional malnutrition analysis (on top of their original 56-page report).
ipcinfo.org/fileadmin/user…
ipcinfo.org/fileadmin/user…



The GoI's claim on mortality analysis completely ignores actual IPC guidance & analysis.
IDF restrictions prevent a comprehensive mortality survey in Gaza.
So the IPC was very up-front that it used an inference approach, and thus declared famine "with reasonable evidence."
IDF restrictions prevent a comprehensive mortality survey in Gaza.
So the IPC was very up-front that it used an inference approach, and thus declared famine "with reasonable evidence."



During the pandemic, it became clear that the CDC lost the mission. It needed a realignment.
More from @US_FDA Commissioner @DrMakaryFDA🧵
More from @US_FDA Commissioner @DrMakaryFDA🧵
It's time to rebuild public trust after the scientific intolerance and extreme partisanship of the Biden Administration.
.@US_FDA is implementing a risk-stratified approach in ending emergency use authorization for COVID-19 vaccines – finally catching America up to the rest of the world.

1/ The 2024 Medicare Shared Savings Program results are released from embargo!
topline results:
10,326,340 bene-years (12% @AledadeACO )
$6,452,075,989 in savings versus benchmark
$4,062,804,612 in payments to ACOs (19% Aledade)
Largest savings ever
Higher quality than FFS🎉
topline results:
10,326,340 bene-years (12% @AledadeACO )
$6,452,075,989 in savings versus benchmark
$4,062,804,612 in payments to ACOs (19% Aledade)
Largest savings ever
Higher quality than FFS🎉
2/ fact sheet:
$643 (2024) vs $515 (2023) in gross per capita savings
Almost 2x savings rate for "low revenue ACOs" (physician-led/FQHC/RHCs) and for those composed predominantly of primary care clinicians vs high revenue ACOs (typically hospital-led)
cms.gov/files/document…
$643 (2024) vs $515 (2023) in gross per capita savings
Almost 2x savings rate for "low revenue ACOs" (physician-led/FQHC/RHCs) and for those composed predominantly of primary care clinicians vs high revenue ACOs (typically hospital-led)
cms.gov/files/document…
3/ How do they get savings?
"lower utilization compared to their benchmark across many categories of utilization including hospital discharges, Emergency Department visits and Skilled Nursing Facility stays"
Better chronic disease management
More prevention
Less suffering
"lower utilization compared to their benchmark across many categories of utilization including hospital discharges, Emergency Department visits and Skilled Nursing Facility stays"
Better chronic disease management
More prevention
Less suffering
Thread incoming on famines & and mortality data.
tl;dr: the Gaza declaration rests on inferred mortality b/c it's impossible to collect good mortality data.
*just like all 3 other famine declarations since 2011*
Meaning no "lowering the bar" for Gaza.
Let’s get into it…
tl;dr: the Gaza declaration rests on inferred mortality b/c it's impossible to collect good mortality data.
*just like all 3 other famine declarations since 2011*
Meaning no "lowering the bar" for Gaza.
Let’s get into it…
A famine declaration assesses food deprivation, malnutrition, and mortality.
In Gaza the food deprivation metric has been clearly met for quite a while.
The malnutrition assessment is solid too (per my earlier threads).
But there is limited data on deaths. So, what to do?
In Gaza the food deprivation metric has been clearly met for quite a while.
The malnutrition assessment is solid too (per my earlier threads).
But there is limited data on deaths. So, what to do?

Famine analyses OFTEN encounter incomplete mortality & other data.
Almost invariably, famine risk arises in context where conflict and political obstacles prevent comprehensive data collection.
In Gaza, mortality data is very poor outside of trauma deaths.
Almost invariably, famine risk arises in context where conflict and political obstacles prevent comprehensive data collection.
In Gaza, mortality data is very poor outside of trauma deaths.
I'm getting a lot of questions about this (false) claim, so let's do a wonky deep dive on how willfully wrong @Israel is on this.
Right off the top: this is the EXACT SAME THRESHOLD that was used in the Sudan famine declaration last year.
Not any lowering of the bar for Gaza.
Right off the top: this is the EXACT SAME THRESHOLD that was used in the Sudan famine declaration last year.
Not any lowering of the bar for Gaza.
The MUAC threshold is used in cases like Sudan or Gaza where access is limited and full weight-for-height studies are not feasible.
Here is the relevant portion of the Dec 2024 famine analysis for Sudan, using the same MUAC >15% threshold. ipcinfo.org/fileadmin/user…
Here is the relevant portion of the Dec 2024 famine analysis for Sudan, using the same MUAC >15% threshold. ipcinfo.org/fileadmin/user…

IPC guidance very explicitly allows for these two approaches to assessing Global Acute Malnutrition in a population:
- weight-for-height analysis
and
- mid-upper-arm circumference (MUAC) screening
MUAC is used when access constraints prevent a full weight-for-height survey.
- weight-for-height analysis
and
- mid-upper-arm circumference (MUAC) screening
MUAC is used when access constraints prevent a full weight-for-height survey.


Starvation in Gaza has been building for months.
The Famine Review Committee conclusion on famine is compelling (more on that below).
Principal responsibility lies with Israeli aid obstruction - but failure of US & Europe to use *any* real leverage on this is also stunning.
🧵
The Famine Review Committee conclusion on famine is compelling (more on that below).
Principal responsibility lies with Israeli aid obstruction - but failure of US & Europe to use *any* real leverage on this is also stunning.
🧵
The evidence for a declaration is persuasive.
There has been evidence of severe food deprivation going back to last year, mainly due to Israeli restrictions.
It got exponentially worse from March '25 onward, after Israel instituted an aid blockade that it has yet to fully lift.
There has been evidence of severe food deprivation going back to last year, mainly due to Israeli restrictions.
It got exponentially worse from March '25 onward, after Israel instituted an aid blockade that it has yet to fully lift.




Malnutrition evidence is also solid, notwithstanding the armchair experts who misread the IPC thresholds.
Say it with me: a MUAC level over 15% is IPC famine territory.
Moreover the rate is continuing to rise to even grimmer levels.
Say it with me: a MUAC level over 15% is IPC famine territory.
Moreover the rate is continuing to rise to even grimmer levels.



For months, folks on this website have pushed a set of "gotcha" tropes to debunk the existence of famine in Gaza.
In fact they are mostly debunking their own credibility on famine dynamics.
As we await tomorrow's IPC report, here is a pre-buttal 🧵of some of those tropes.
In fact they are mostly debunking their own credibility on famine dynamics.
As we await tomorrow's IPC report, here is a pre-buttal 🧵of some of those tropes.
Most of this denialism comes from armchair experts who have never worked on hunger emergencies.
FWIW, I directed USG famine prevention efforts for:
- South Sudan 2013-14
- Yemen 2015-16
- Ethiopia 2016
- Nigeria 2016
Plus a lot of smaller ones.
On to the gotchas...
FWIW, I directed USG famine prevention efforts for:
- South Sudan 2013-14
- Yemen 2015-16
- Ethiopia 2016
- Nigeria 2016
Plus a lot of smaller ones.
On to the gotchas...
Gotcha 1: This starving kid is next to a parent who isn't starving! Clearly a ruse!
Why it’s BS: The nutritional needs of growing children make them far more vulnerable to starvation than adults. They invariably starve earlier.
Good overview here: telegraph.co.uk/global-health/…
Why it’s BS: The nutritional needs of growing children make them far more vulnerable to starvation than adults. They invariably starve earlier.
Good overview here: telegraph.co.uk/global-health/…


In new study led by Bernadeta Dadonaite, we measure how spike mutations affect function & antigenicity of spike of KP.3.1.1 strain of SARS-CoV-2.
Sheds light on how key neutralizing epitopes are changing & importance of RBD up/down motion.
biorxiv.org/content/10.110…
Sheds light on how key neutralizing epitopes are changing & importance of RBD up/down motion.
biorxiv.org/content/10.110…
We examined spike of KP.3.1.1, a strain from late 2024 / early 2025 similar to current variants
KP.3.1.1 & other recent variants have >60 spike amino-acid mutations relative to early pandemic strains, as spike has evolved at extraordinary rate of >10 mutations/year on avg
KP.3.1.1 & other recent variants have >60 spike amino-acid mutations relative to early pandemic strains, as spike has evolved at extraordinary rate of >10 mutations/year on avg

We previously developed pseudovirus deep mutational scanning (), which uses non-replicative viral particles to safely study spike mutations.
Here we used approach to measure how mutations to KP.3.1.1 spike affect five phenotypes, as shown below. pubmed.ncbi.nlm.nih.gov/36868218/
Here we used approach to measure how mutations to KP.3.1.1 spike affect five phenotypes, as shown below. pubmed.ncbi.nlm.nih.gov/36868218/


As I wrote in SUPER AGERS, the immune system is the key to modulating our aging process and the opportunity to extend healthspan. Today @NatureAging 7 new articles, summarized here, that reinforce its central role
nature.com/articles/s4358…
nature.com/articles/s4358…


The potential consequences of too youthful immune system in an older person —> autoimmunity
nature.com/articles/s4358…
nature.com/articles/s4358…

.@NBCNews claims that @SecKennedy's recommendation to fry potatoes in beef tallow - rather than the seed oils used today - "isn’t backed by scientific research."
Here is a basketful of studies that tell a different story: 🍟1/7
Here is a basketful of studies that tell a different story: 🍟1/7
First, some context:
• Beef tallow, rendered suet from a cow, is known to contain high levels of saturated fatty acids (SFAs), which can also be found in coconut oil and dairy products.
• Ultra-processed seed oils, such as those derived from rapeseeds ("canola") and soybeans, contain higher levels of polyunsaturated fatty acids (PUFAs). 🍟2/7
• Beef tallow, rendered suet from a cow, is known to contain high levels of saturated fatty acids (SFAs), which can also be found in coconut oil and dairy products.
• Ultra-processed seed oils, such as those derived from rapeseeds ("canola") and soybeans, contain higher levels of polyunsaturated fatty acids (PUFAs). 🍟2/7
Foods such as wild blueberries and carrots are praised for their high levels of antioxidants, which have been shown to protect the human body from the free radicals linked to many chronic health conditions.
By contrast, the PUFAs found in seed oils are "particularly susceptible to oxidative damage" and produce "aldehydes," which "exert a range of toxicological effects," during the frying process.
(Haywood et al., 1994) 🍟3/7
pubmed.ncbi.nlm.nih.gov/7633572/
By contrast, the PUFAs found in seed oils are "particularly susceptible to oxidative damage" and produce "aldehydes," which "exert a range of toxicological effects," during the frying process.
(Haywood et al., 1994) 🍟3/7
pubmed.ncbi.nlm.nih.gov/7633572/
Always illuminating to check whether accounts using other crises to downplay Gaza have *ever* otherwise shown concern about those crises.
Almost invariably: nope. Just a clumsy, cynical attempt to dunk on Gaza activism.
Let's dive into the levels of bad faith at play here:
🧵
Almost invariably: nope. Just a clumsy, cynical attempt to dunk on Gaza activism.
Let's dive into the levels of bad faith at play here:
🧵
First, the receipts:
@IsraelMFA has NEVER before shown concern about the humanitarian crises in Sudan: x.com/search?q=sudan…
or Afghanistan: x.com/search?q=afgha…
or DR Congo: x.com/search?q=congo…
or Yemen: x.com/search?q=yemen…
It just wants to use them as props.
@IsraelMFA has NEVER before shown concern about the humanitarian crises in Sudan: x.com/search?q=sudan…
or Afghanistan: x.com/search?q=afgha…
or DR Congo: x.com/search?q=congo…
or Yemen: x.com/search?q=yemen…
It just wants to use them as props.
That's pretty grotesque in its own right.
But now let's check how much the government of Israel has donated to those same crises over the past few years.
From everything I can find, the answer seems to be:
*zero*
But now let's check how much the government of Israel has donated to those same crises over the past few years.
From everything I can find, the answer seems to be:
*zero*
The new special issue @ScienceMagazine features Immunity with 4 outstanding review papers, 5★
Our immune system over the lifespan, sex differences, influence on physiology, and host antiviral defenses science.org/toc/science/cu…
Our immune system over the lifespan, sex differences, influence on physiology, and host antiviral defenses science.org/toc/science/cu…

Our immune system as we age: the path to immunosenesence and inflammaging
science.org/doi/10.1126/sc…
science.org/doi/10.1126/sc…

Sex differences science.org/doi/10.1126/sc…

The world's famine alert system is warning us – in the starkest possible terms – that any remaining window to avert mass starvation deaths in Gaza is about to close.
A quick dive into what the report tells us:
A quick dive into what the report tells us:
This confirms what media reports (and frankly anyone with eyes) could see over the past week: a famine unfurling in Gaza.
While this is not (yet) a formal famine declaration, it signals that one is likely coming.
Importantly, formal declarations ALWAYS come after the fact.
While this is not (yet) a formal famine declaration, it signals that one is likely coming.
Importantly, formal declarations ALWAYS come after the fact.
Famine declaration is a lagging indicator.
By the time data can be collected proving the presence of famine conditions, those conditions have invariably been in place for some time.
In the 2011 Somalia famine, half of the 260K people lost had already died prior to declaration.
By the time data can be collected proving the presence of famine conditions, those conditions have invariably been in place for some time.
In the 2011 Somalia famine, half of the 260K people lost had already died prior to declaration.
Netanyahu has used aid diversion claims as pretext for massive obstruction of aid to Gaza.
Now we learn the IDF had briefed his team that these claims were false (as aid groups have long argued).
This constitutes further evidence he is using starvation as a weapon of war.
🧵
Now we learn the IDF had briefed his team that these claims were false (as aid groups have long argued).
This constitutes further evidence he is using starvation as a weapon of war.
🧵
Humanitarian groups have long denied that their aid is being diverted at any significant scale.
My organization dug into this last year and found no evidence for the Israeli govt claims. refugeesinternational.org/reports-briefs…
My organization dug into this last year and found no evidence for the Israeli govt claims. refugeesinternational.org/reports-briefs…
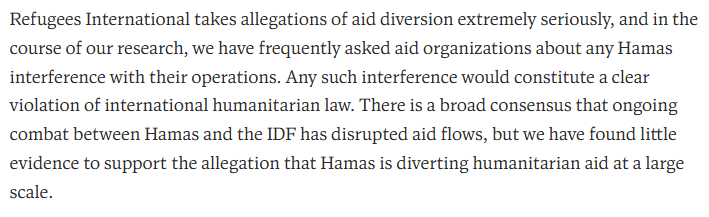
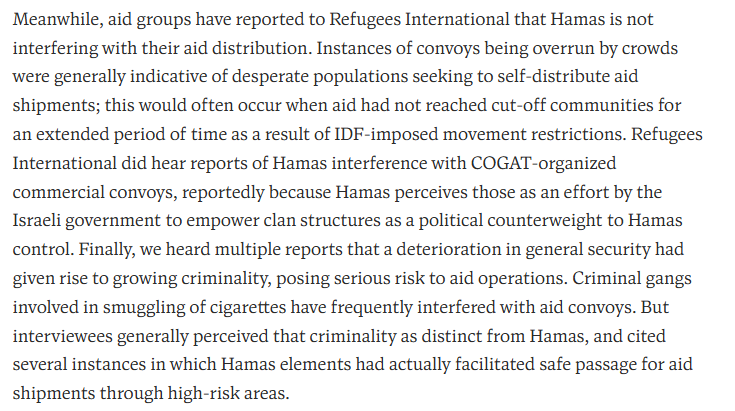
US envoy David Satterfield - a savvy, hard-nosed diplomat and no one's idea of a bleeding heart - has consistently said the same.
As a longtime humanitarian who has battled famines and hunger crises, I fear that starvation in Gaza has now passed the tipping point and we are going to see mass-scale starvation mortality.
A thread on famine momentum, famine response, and what it means for Gaza today.
A thread on famine momentum, famine response, and what it means for Gaza today.
The latest reporting shows telltale signs of rapidly accelerating mortality - the kind of classic famine scenario we know from places like Sudan or Somalia.
Barring a massive reversal of Israeli policy, there is a little standing in the way of total collapse.
Barring a massive reversal of Israeli policy, there is a little standing in the way of total collapse.
Throughout last year Gaza ebbed and flowed at the brink of famine, but never passed the tipping point.
Israeli aid obstruction kept Palestinians perpetually underfed but always relented just enough to avoid mass hunger mortality, as we wrote last Sept:
refugeesinternational.org/reports-briefs…
Israeli aid obstruction kept Palestinians perpetually underfed but always relented just enough to avoid mass hunger mortality, as we wrote last Sept:
refugeesinternational.org/reports-briefs…


Amid all the noise, it can be hard to figure out the facts of the Epstein-Trump relationship.
Here is a year-by-year timeline thread summarizing their connections (with sourcing and documentation) from 1990 until present.
🧵 1/17
Here is a year-by-year timeline thread summarizing their connections (with sourcing and documentation) from 1990 until present.
🧵 1/17
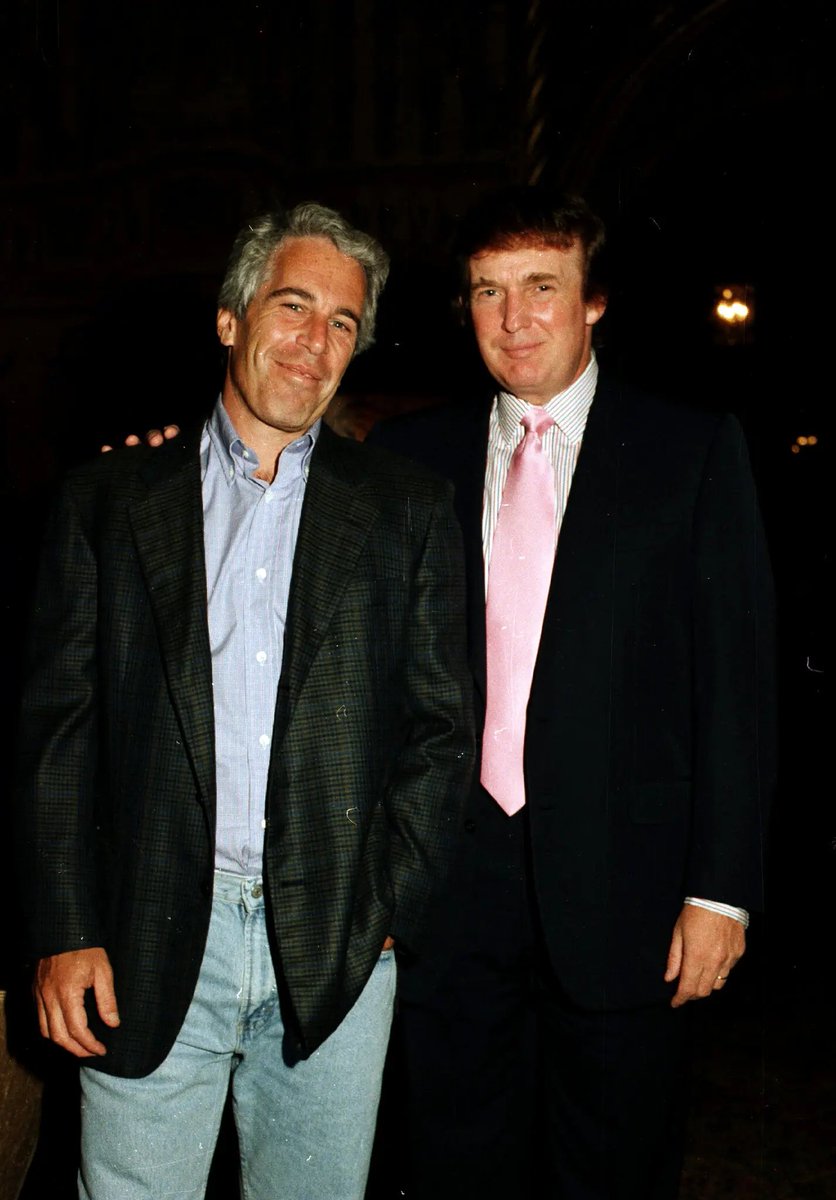
1990: Epstein buys a property two miles north of Mar-a-Lago.
Two years later, in 1992, NBC video shows Epstein and Trump partying at Mar-a-Lago at an event featuring Buffalo Bills cheerleaders.
2/17
Two years later, in 1992, NBC video shows Epstein and Trump partying at Mar-a-Lago at an event featuring Buffalo Bills cheerleaders.
2/17
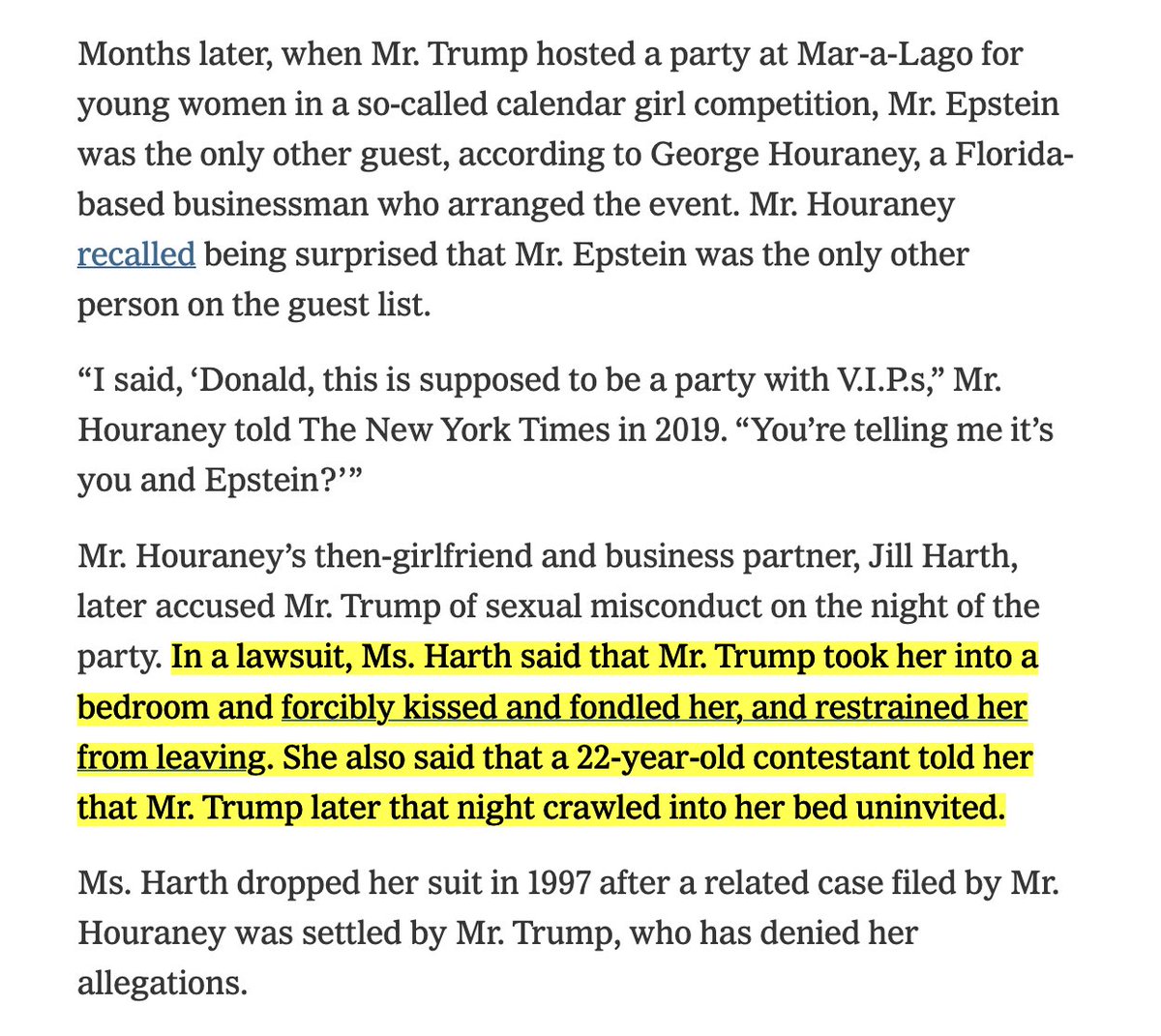
Weeks later, still in 1992, another Mar-a-Lago party was for a "calendar girl" competition. Epstein and Trump were there.
Jill Harth later accused Mr. Trump of sexual assaulting her that night. Trump denied the allegations.
3/17 nytimes.com/2025/07/19/us/…
Jill Harth later accused Mr. Trump of sexual assaulting her that night. Trump denied the allegations.
3/17 nytimes.com/2025/07/19/us/…
We have been mapping and studying the known flood risks at Camp Mystic.
It turns out that not only was the camp in a flood zone, some cabins were located in areas that local county officials had deemed “extremely hazardous.”
Here is more of what we found.
🧵 1/9
It turns out that not only was the camp in a flood zone, some cabins were located in areas that local county officials had deemed “extremely hazardous.”
Here is more of what we found.
🧵 1/9
The riskiest areas are known as “floodways,” where rushing waters are expected during flood events.
In Kerr County, like many places, officials put strict limits on development in those areas “to protect human life.”
Story link:
2/9 nytimes.com/interactive/20…
In Kerr County, like many places, officials put strict limits on development in those areas “to protect human life.”
Story link:
2/9 nytimes.com/interactive/20…

We found that Camp Mystic had 6 cabins in the floodway, including those housing some of the youngest campers. Other camp buildings were also in that part of the flood zone.
3/9
3/9

Texas officials have long worried about the dangers to children who packed into camps each summer along the flood-prone Guadalupe River. They knew that warning systems were inadequate.
So why was nothing done? We have reviewed documents spanning a decade to find answers.
🧵 1/9
So why was nothing done? We have reviewed documents spanning a decade to find answers.
🧵 1/9
Without a more advanced warning system, the youth camps on the river had instead relied on a word-of-mouth strategy: Upstream camps would warn downstream peers of water surges coming their way.
2/9
nytimes.com/2025/07/06/us/…
2/9
nytimes.com/2025/07/06/us/…
But officials repeatedly wondered whether that was sufficient.
Here's a county commissioner talking in 2017, during a discussion about river gauges, sirens, and other ways the might alert people to flash floods.
3/9
Here's a county commissioner talking in 2017, during a discussion about river gauges, sirens, and other ways the might alert people to flash floods.
3/9


STAGGERING: This new study of 133 countries is the first to estimate the impact of all USAID’s work. In 2 decades, it saved *92M* lives.
Current cuts, if not reversed, are forecast to cost *14M* lives thru 2030.
thelancet.com/journals/lance…
Current cuts, if not reversed, are forecast to cost *14M* lives thru 2030.
thelancet.com/journals/lance…

Higher USAID support was associated w a 15% reduction in overall deaths and 32% reduction in child deaths.
This wasn't just due to its health work but also its development support for economies, people, and institutions that transitioned numerous countries off of aid.
This wasn't just due to its health work but also its development support for economies, people, and institutions that transitioned numerous countries off of aid.

Today, what’s left of USAID is being transferred to the State Dept, which is gutting that development work.
Ending USAID will go down in history as a colossal failure and mistake.
Ending USAID will go down in history as a colossal failure and mistake.
NEW: There is a fascinating political drama unfolding right now at Indian Creek Village, the small gated island known as the “Billionaire Bunker,” home to the likes of Jeff Bezos, Tom Brady and Ivanka Trump.
It is a saga revolving around the island's 💩
THREAD (1/8)
It is a saga revolving around the island's 💩
THREAD (1/8)

Despite the island’s extreme luxury (an empty lot sold for $110M), Indian Creek does not have a sewer system. The island proposed sending waste into the pipes of neighboring Surfside but then balked at the town’s $10M ask.
That was just the start.
(2/8)
nytimes.com/2025/06/13/us/…
That was just the start.
(2/8)
nytimes.com/2025/06/13/us/…
One of Indian Creek’s residents called the $10 million fee a “shakedown.” Another called it “extortion.” The village attorney called it a “ransom.”
(3/8)
nytimes.com/2025/06/13/us/…
(3/8)
nytimes.com/2025/06/13/us/…


I've been thinking on my review of RFK Jrs 8 new ACIP members
When announced, I found myself thinking "could've been much worse" and so was relatively favorable
However, the bar being set so low caused me to miss a huge piece... and there's still great risk!
Short thread
1)
When announced, I found myself thinking "could've been much worse" and so was relatively favorable
However, the bar being set so low caused me to miss a huge piece... and there's still great risk!
Short thread
1)
While I was pretty favorable to a majority of the new members - the bar is set inredibly low -
I was just happy the 8 were not the most hard core ideologues for whom destroying vaccines is practically religion (like RFK Jr)
That obscured the biggest problem of the group
2/
I was just happy the 8 were not the most hard core ideologues for whom destroying vaccines is practically religion (like RFK Jr)
That obscured the biggest problem of the group
2/
Perhaps the biggest problem is it is a panel of people who, generally speaking, are generally NOT:
experts in diseases vaccines prevent
experts in vaccines
infectious disease epidemiology
clinical trials
If this was the private sector, no way would this group pass muster
3/
experts in diseases vaccines prevent
experts in vaccines
infectious disease epidemiology
clinical trials
If this was the private sector, no way would this group pass muster
3/
RFK Jr released names of 8 ppl he is placing into ACIP to replace 17 removed
Actually a majority are v reasonable - 2 of 8 however align heavily w conspiracy & anti-vax but as I discuss, their presence may have a silver lining
My thoughts:
Thread
1/cnbc.com/amp/2025/06/11…
Actually a majority are v reasonable - 2 of 8 however align heavily w conspiracy & anti-vax but as I discuss, their presence may have a silver lining
My thoughts:
Thread
1/cnbc.com/amp/2025/06/11…
Joseph Hibbeln MD has long researched and advocated for optimizing nutrition, including studying things like seafood consumption in pregnancy and role of mercury consumption and whether it is linked to autism. Generally he’s come out saying it’s not.
Summary: No evidence of anti science or anti vaccine. Likely very balanced and nuanced rigorous scientist to serve on ACIP.
2/
Summary: No evidence of anti science or anti vaccine. Likely very balanced and nuanced rigorous scientist to serve on ACIP.
2/
Cody Meissner MD
Is a pediatric infectious disease expert at my Alma mater - Dartmouth. He is a rigorous scientist and has defended vaccines while formally recognizing underlying issues that are causing people to turn away from them - such as vaccine success driving down disease - affording people the luxury of focusing on very rare side effects while forgetting the real impacts of the diseases.
For example in @NEJM he wrote:
Summary. Terrific Choice
3/
Is a pediatric infectious disease expert at my Alma mater - Dartmouth. He is a rigorous scientist and has defended vaccines while formally recognizing underlying issues that are causing people to turn away from them - such as vaccine success driving down disease - affording people the luxury of focusing on very rare side effects while forgetting the real impacts of the diseases.
For example in @NEJM he wrote:
Summary. Terrific Choice
3/
