
1/ In Dec. 2018, I posted my first #Tweetorial, on digestive tract neuroendocrine neoplasms. I polled Twitter asking what my next topic would be, and the winner was hepatic masses. More than a YEAR later, here it is! #pathology #liverpath
2/ Broad points: Most liver masses are benign, especially in younger patients. Older and cirrhotic patients are at increased risk for malignancy. Masses in cirrhosis are almost always primary liver malignancies (usually HCC).
3/ Don’t forget mets! All blood filters through the liver, so it’s prime real estate for metastatic disease … unless cirrhotic, in which case mets are rare. Pictured are two unusual liver mets: chordoma and medullary thyroid carcinoma. 


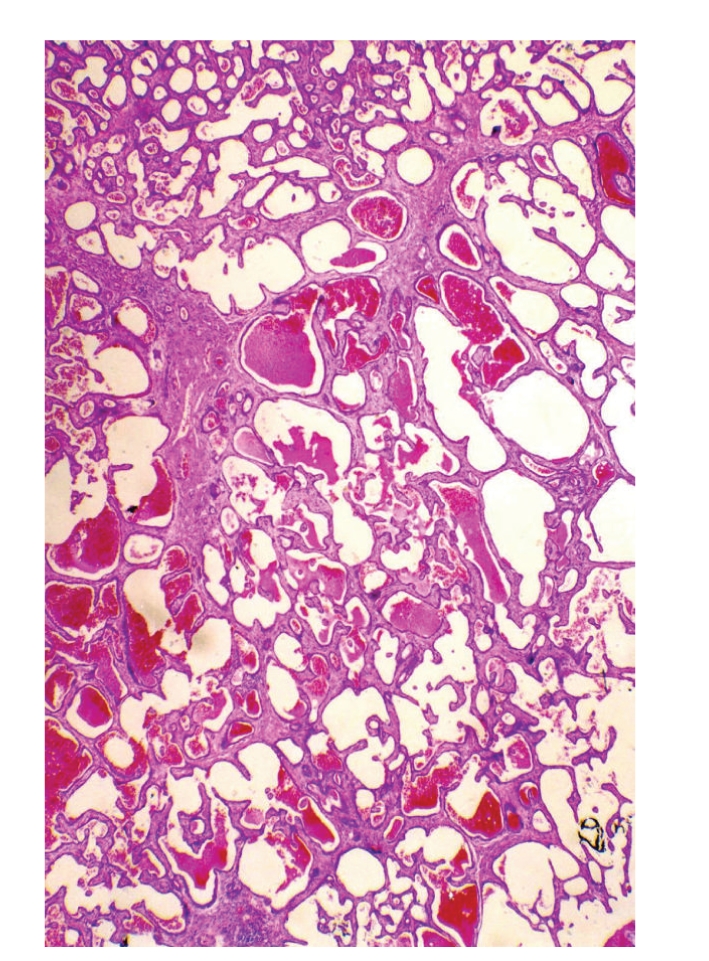
4/ OK, on to primary lesions. Going to go by category and start with vascular. The most common hepatic mass, of course, is the humble cavernous hemangioma. Benign, usually solitary, wide size range. Won’t burst or become malignant.

5/ The new WHO 5th edition formally recognizes some variants, including diffuse hepatic hemangiomatosis, hepatic small vessel neoplasm, and anastomosing hemangioma (AH). Those last two may be the same thing? AH pic courtesy @CerubbSilva.
6/ Another hemangioma variant is the infantile hemangioma (aka hemangioendothelioma). Patients usually < 6 months old. Benign, but can cause CHF or platelet consumption. Orderly small vessels, background connective tissue.



7/ Another peds vascular lesion is congenital hepatic vascular malformation. May look more malformation-y, with more dilated and spaced-out vessels. They are GLUT1-negative, unlike infantile hemangioma (helpful if H&E morphology overlap).


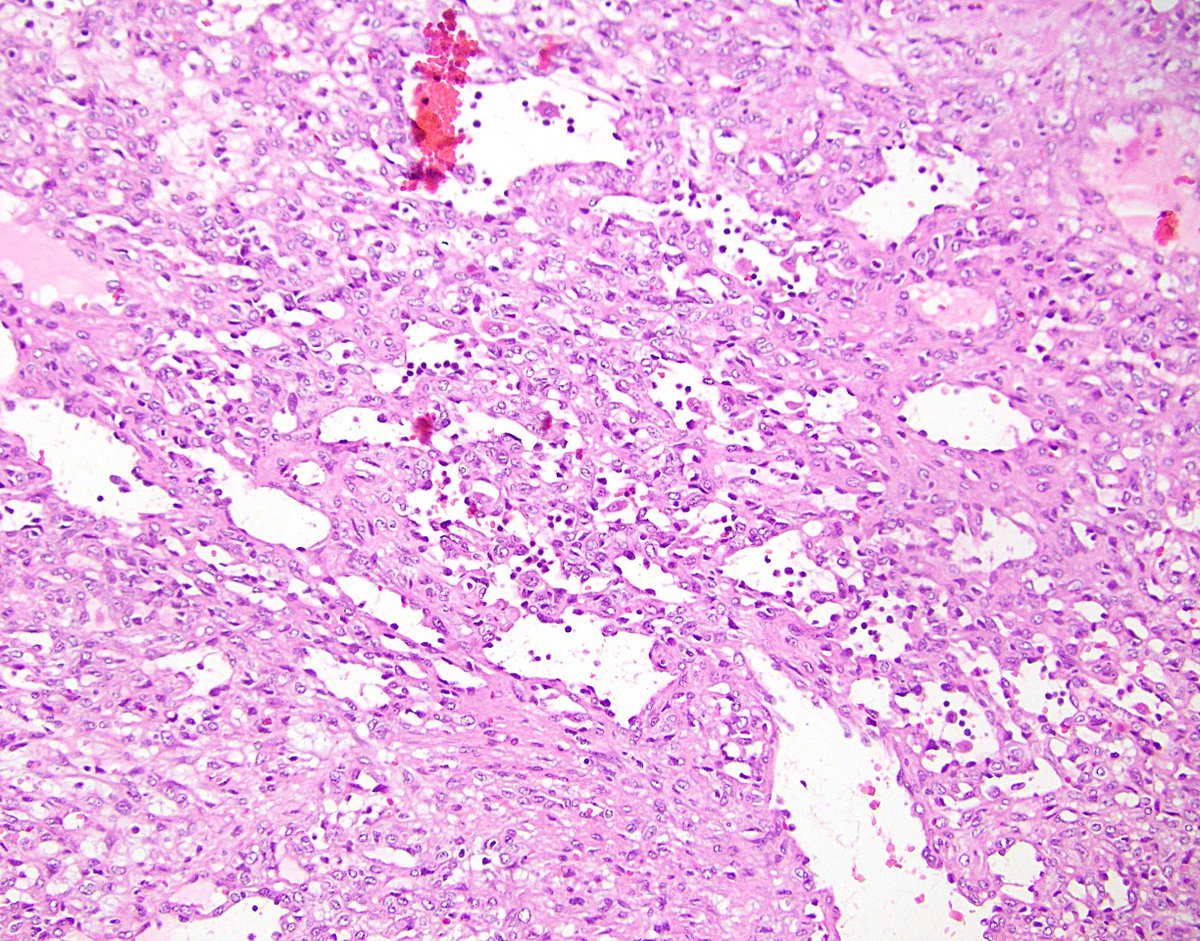
8/ Now we’re getting into the bad actors. Epithelioid hemangioendothelioma (EHE) is often multifocal and can occur anywhere in the body. More common in women. Small vessels, blister cells (“single cell vessels”), myxoid background.


9/ Most cases of EHE have a WWTR1-CAMTA1 fusion, with corresponding nuclear CAMTA1 IHC positivity. Rare cases have YAP1-TFE3 instead and are positive for TFE3.
10/ Finally, of course, angiosarcoma. Malignant vascular neoplasm. Rare in liver. Linked to thorotrast use, so if you see a hepatic angiosarcoma in someone that’s 120 years old, give that a thought …


11/ Starting biliary masses w/ the humble bile duct hamartoma (von Meyenburg complex). Common. Benign. Don’t mistake it for metastatic carcinoma on frozen! Small, angled ducts with inspissated bile. Multifocal in ducal plate malformations.


12/ Bile duct adenoma is also benign. A bit bigger than hamartomas (but usually <0.5 cm), and more tightly packed. Often inflammation around the periphery. Probably does not progress to cholangiocarcoma.


13/ A similar but super-rare lesion is biliary adenofibroma. (Never seen one -- pics from bit.ly/2v8qc4M) Large, solid/microcystic, can have malignant foci. Basically looks like a bigger, badder version of the past two entities.
14/ Mucinous cystic neoplasm of the liver (formerly biliary cystadenoma) resembles its more-common pancreatic counterpart. More common in women, mucinous lining, surrounding ovarian-type stroma, may progress to malignancy.


15/ And now, cholangiocarcinoma, the “adenocarcinoma of the liver.” Most common in Southeast Asia. Risk factors include cirrhosis, liver fluke infection, and primary sclerosing cholangitis (but not primary biliary cirrhosis).
16/ It can form several gross patterns including mass-forming, periductal infiltrating, and intraductal. This used to matter for AJCC staging but no longer does!
17/ There are 2 distinct subtypes of intrahepatic cholangiocarcinoma. Large duct type arises in biliary disease and shows precursor lesions, mucin production, perineural invasion, likely worse survival, and KRAS and SMAD4 abnormalities.

18/ In contrast, the small duct type arises in hepatic disease, creates sclerosis more than desmoplasia, and has IDH1/IDH2 abnormalities. Cholangiolocarcinoma (2nd pic) is now considered this, rather than a combined HCC-cholangiocarcinoma.


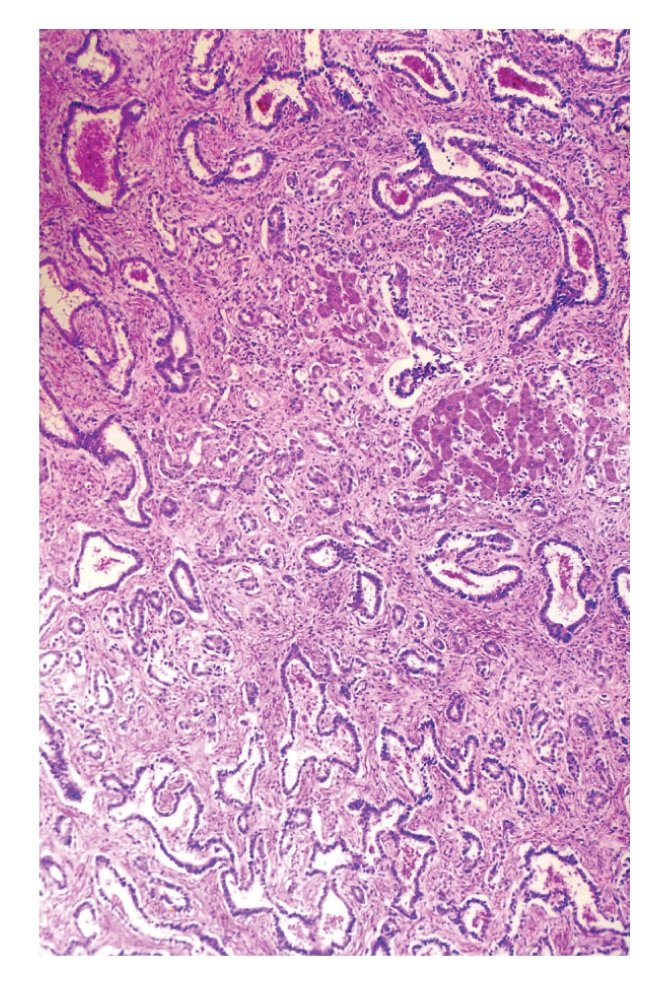
19/ Now to hepatocellular masses, starting with focal nodular hyperplasia (FNH). Not a neoplasm! Likely a localized response to abnormal blood flow. Central scar, dilated vessels, ductular reaction, bland hepatocellular nodules.



20/ The confusion (or fun) really begins with hepatocellular adenoma (HCA). Not that uncommon, usually arising in younger women on oral contraceptives. Can be large, can be multifocal, can rupture. Rarely turns malignant. So many subtypes!
21/ Probably the most common HCA subtype is the HNF1A-inactivated form. Tumors (and patients) are usually fatty. The key to this (and all) HCA is unpaired arteries. Reticulin may show mildly thickened cell plates. No atypia.


22/ Next most common is inflammatory (also sometimes called telangiectatic) HCA. Sprinkling of inflammation, dilated sinusoids. Often positive for serum amyloid A or C-reactive protein by IHC. (See those lovely unpaired arteries?)

23/ The third type is beta-catenin-mutated. This type is more common in men and higher risk of progression to hepatocellular carcinoma. Some cases show pseudoacinar arrangement and focal nuclear atypia.

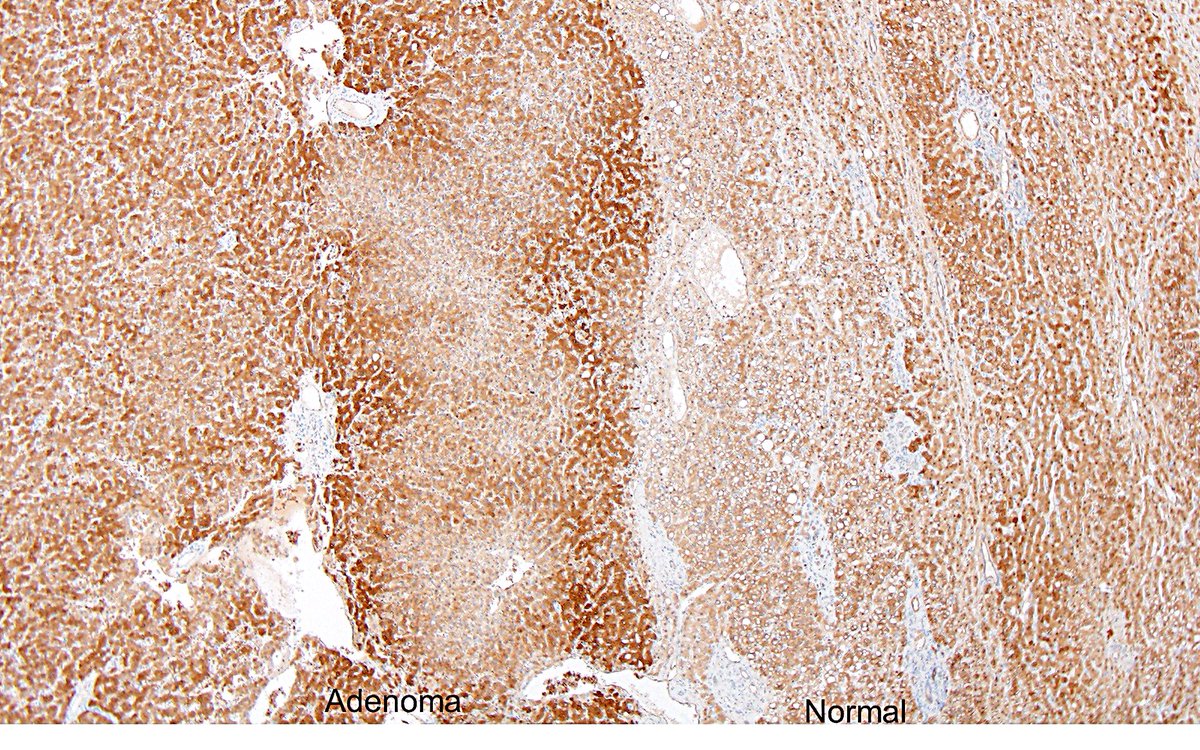
24/ IMPORTANT – inflammatory HCA can also have mutated beta-catenin! Always get beta-catenin IHC on HCAs (look for nuclear staining; may be focal.) Glutamine synthetase can also be helpful; diffuse staining suggests beta-catenin mutation.

25/ The final, vaguely defined HCA subtype is the sonic hedgehog variety. These are uncommon and tend to bleed. ASS1 IHC may help identify them (hey look, it’s the urea cycle!), but data are conflicting. Photo courtesy @rondell_graham.
26/ Large, bland, prominent hepatocellular nodules that are not HCA have confusing terminology. In cirrhosis? Macroregenerative nodule. In abnormal flow states? Large regenerative nodule. Morphology is the same. (I think I got this right…)

27/ And on to hepatocellular carcinoma (HCC). Most common hepatic liver malignancy, 5th most common cancer worldwide. It typically arises in cirrhosis of any cause, though it can occur in non-cirrhotic livers (one cause: HBV).
28/ Classic HCC features include expanded plates and endothelial wrapping (particularly on cytology specimens). Well-differentiated lesions are clearly hepatocellular, while poorly differentiated ones require IHC (HepPar1, glypican3).



29/ Be sure to look carefully for lymphovascular invasion, as this can upstage some HCC (and also cholangiocarcinoma).

30/ If a liver lesion meets LI-RADS criteria, it does NOT have to be sampled to establish the dx of HCC! This is great, in part because well-differentiated hepatocellular lesions can be quite tricky on small samples. Reticulin may help.



31/ Several subtypes of HCC have been described, with many added in the latest WHO. They include clear cell HCC (pic 1), steatohepatitic HCC (pic 2), scirrhous HCC (pic 3), and sarcomatoid HCC (pic 4).




32/ The most famous HCC subtype is also @rondell_graham’s favorite – fibrolamellar HCC! Has a central scar, just like FNH. Usually in younger, non-cirrhotic patients. Eosinophilic cells, prominent nuclei, fibrosis. DNAJB1-PRKACA fusion.
33/ So where does HCC come from? Namely, how do we get from the first picture to the second, then to the third?



34/ Some HCC arise in HCA, as above. More often, dysplastic nodules arise in cirrhotic livers, then progress to HCC. These can be low-grade (pictured) or high-grade. Never hurts to look for them when you’re studying a resection specimen.

35/ Now to wander into combined HCC-cholangiocarcinoma. This concept and classification remain in flux. The current WHO does not define subtypes, instead simply requiring unequivocal hepatocytic and cholangiocytic differentiation on H&E.
36/ Here are a few photos of various “types” of combined HCC-cholangiocarcinoma, including a collision-like lesion (pic 1), a “stem cell” type (pic 2), and an intermediate cell carcinoma (pic 3).



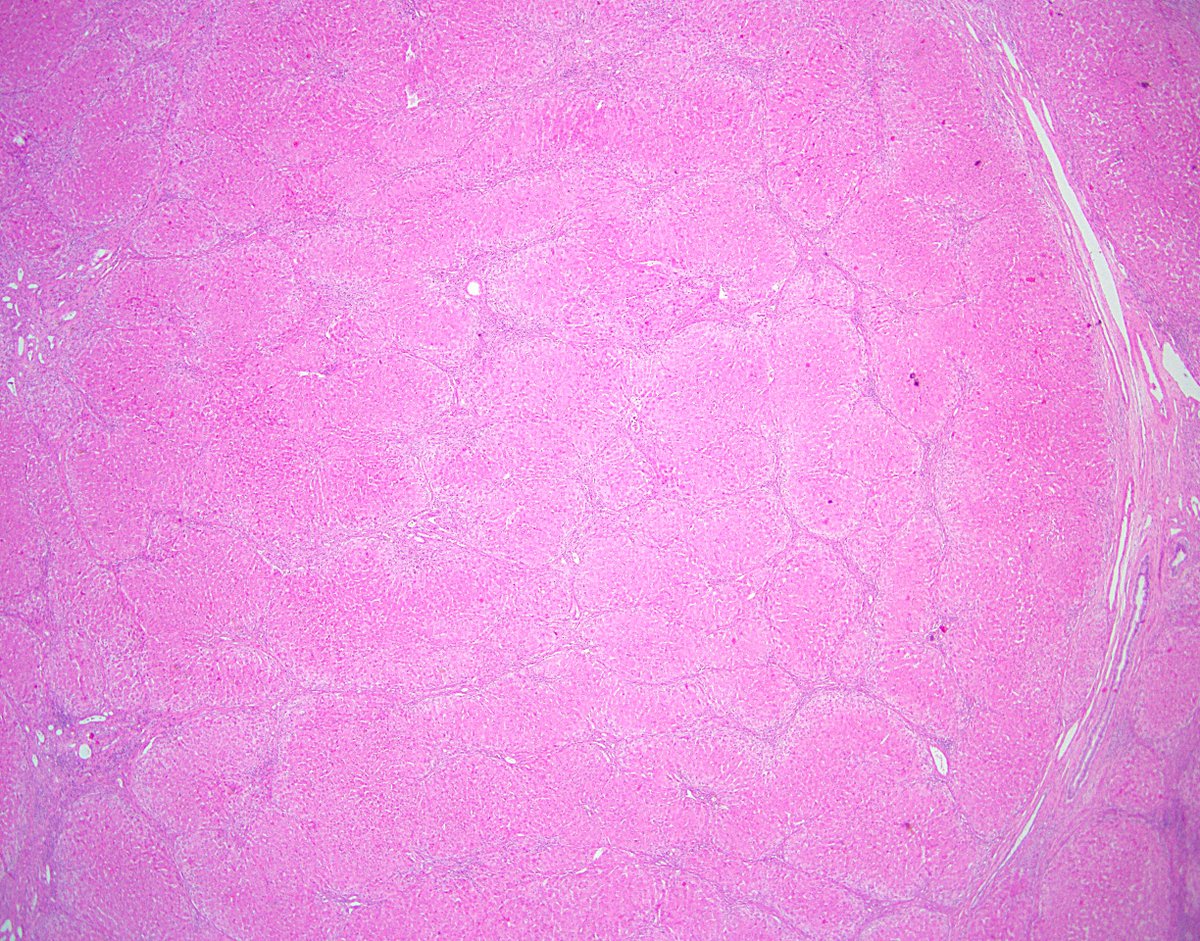
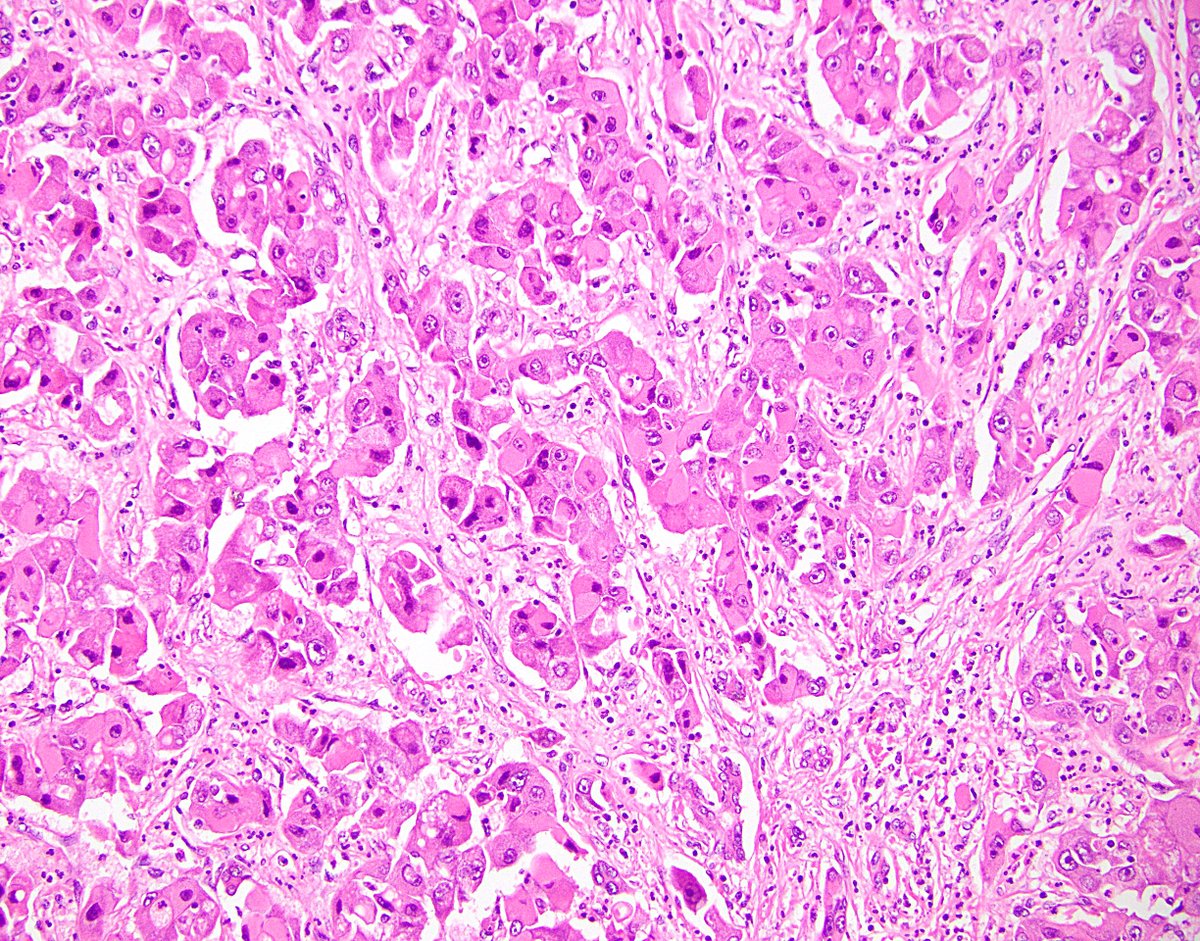
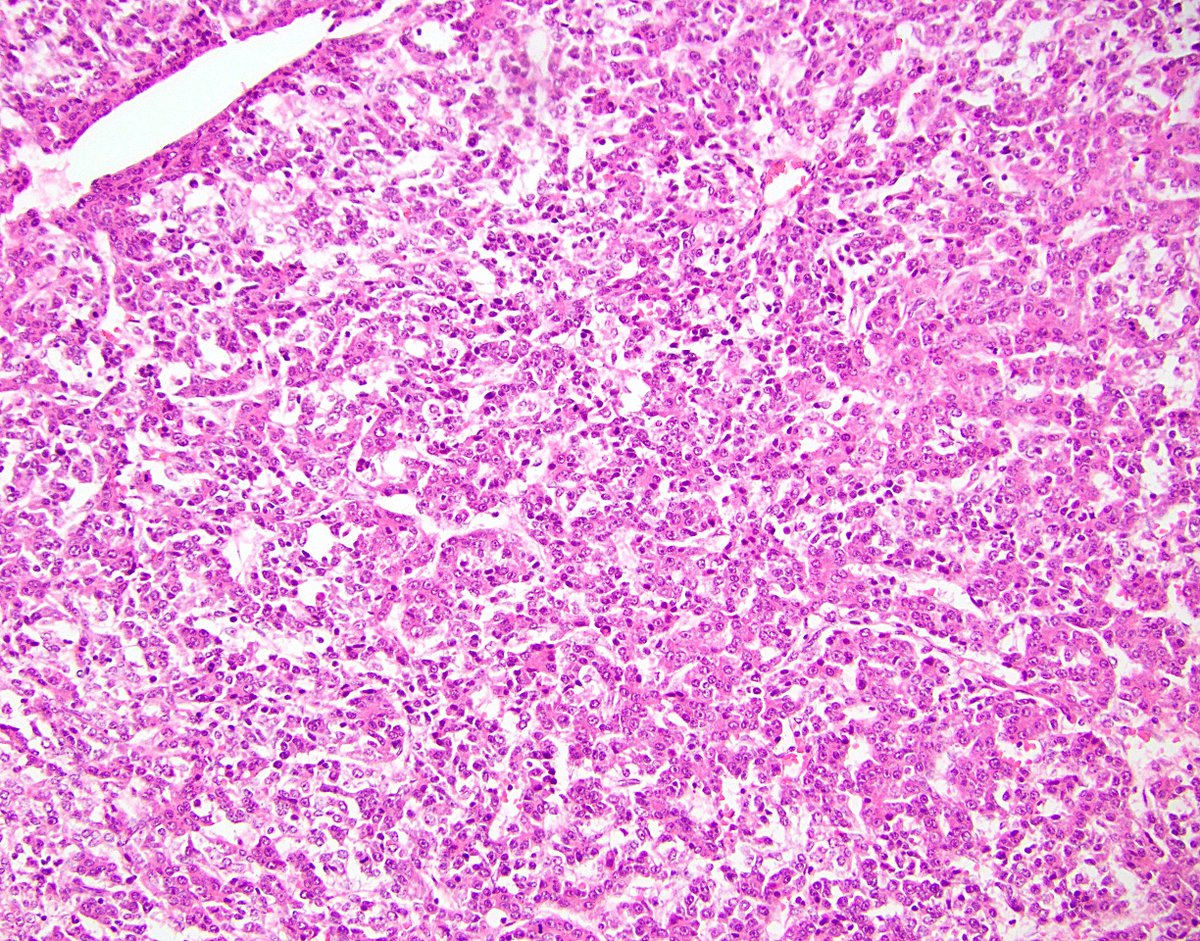
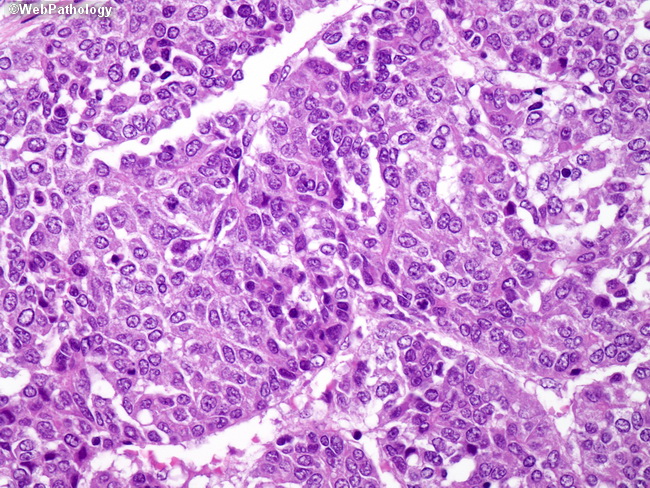
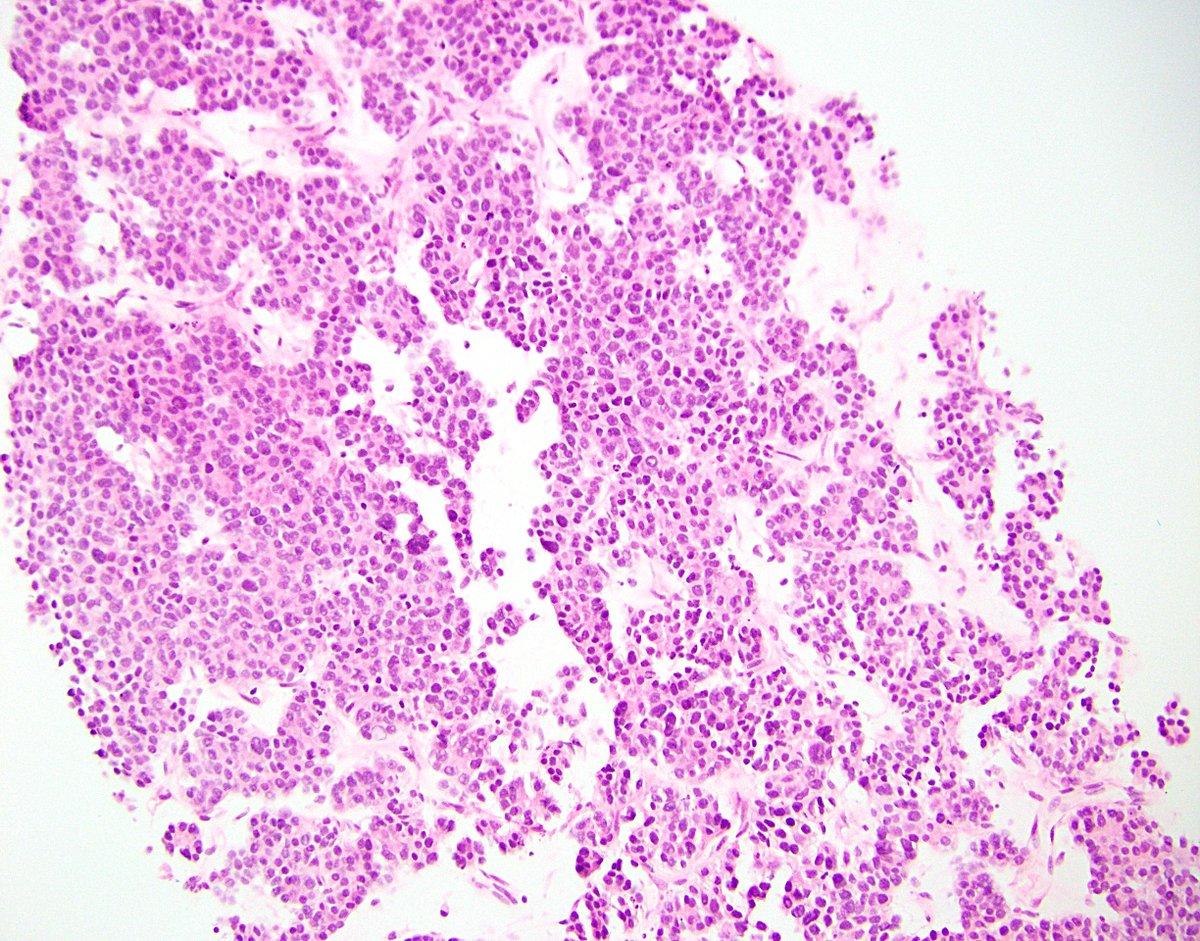
37/ Finally, hepatoblastoma. (I’m not a peds pathologist and I never see these.) Most common liver tumor, mostly in children under age 5. Linked to many syndromes (FAP, Beckwith–Wiedemann, etc.). COG staging system, based on resectability.
38/ Many histologic subtypes, including fetal (pic 1), embryonal (pic 2), mixed epithelial-mesenchymal (pic 3), and teratoid (pic 4). Pics 2-4 taken from the amazing resource @WebPathology.
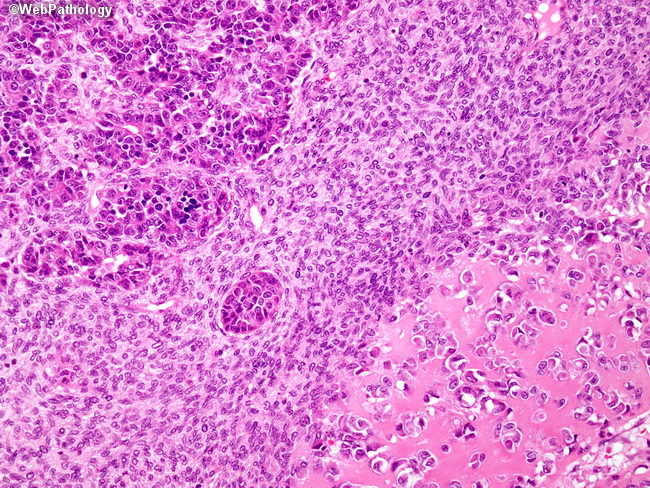
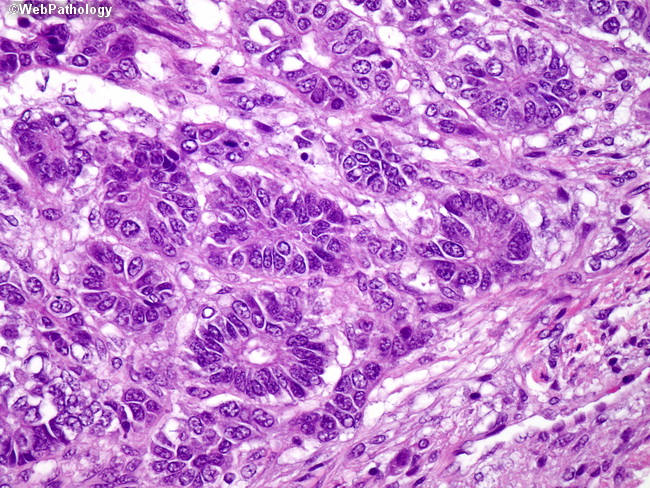
39/ I’ll now talk about mesenchymal (and mesenchymal-ish lesions). Easy one to start – focal fatty change. Name says it all. Not linked to obesity. Don’t mistake for a hepatocellular adenoma.

40/ Also something not to mistake for a hepatocellular adenoma, or carcinoma, is angiomyolipoma. Similar to the kidney lesion. Often epithelioid. A small percentage arise in tuberous sclerosis pts. IHC for SMA and HMB45 confirms the dx.


41/ Mesenchymal hamartoma is an uncommon, benign pediatric liver lesion (median age: 15 months). Disorganized mess of hepatocyte and biliary elements, in a myxoid stroma.


42/ Undifferentiated (embryonal) sarcoma is a rare, nasty mesenchymal malignancy of the liver. Third most common peds liver cancer (usually age 6-10). High-grade, primitive, myxoid background, PAS-positive globules. Therapy works well-ish.
43/ Calcifying nested stromal-epithelial tumor is super fun (for pathologists) and super rare. Name has changed a few times, but the current one is nicely descriptive. Biphasic. CTNNB1 (beta-catenin) mutations. Good prognosis overall!

44/ There purportedly exists an aggressive lesion called transitional liver cell tumor. Extremely few cases reported, mostly in children. I’ve never seen one. I think some peds pathologists doubt it actually exists. It’s not in the new WHO.
45/ And, of course, mesenchymal “soft tissue” lesions that occur elsewhere in the body may also arise in the liver. To demonstrate: solitary fibrous tumor (pic 1), inflammatory myofibroblastic tumor (pic 2), leiomyosarcoma (pic 3).



46/ Neuroendocrine tumors often metastasize to the liver. Very rarely, it appears they can arise as a liver primary. This is official in the new WHO. To make this diagnosis, a primary lesion from another site must be convincingly excluded.

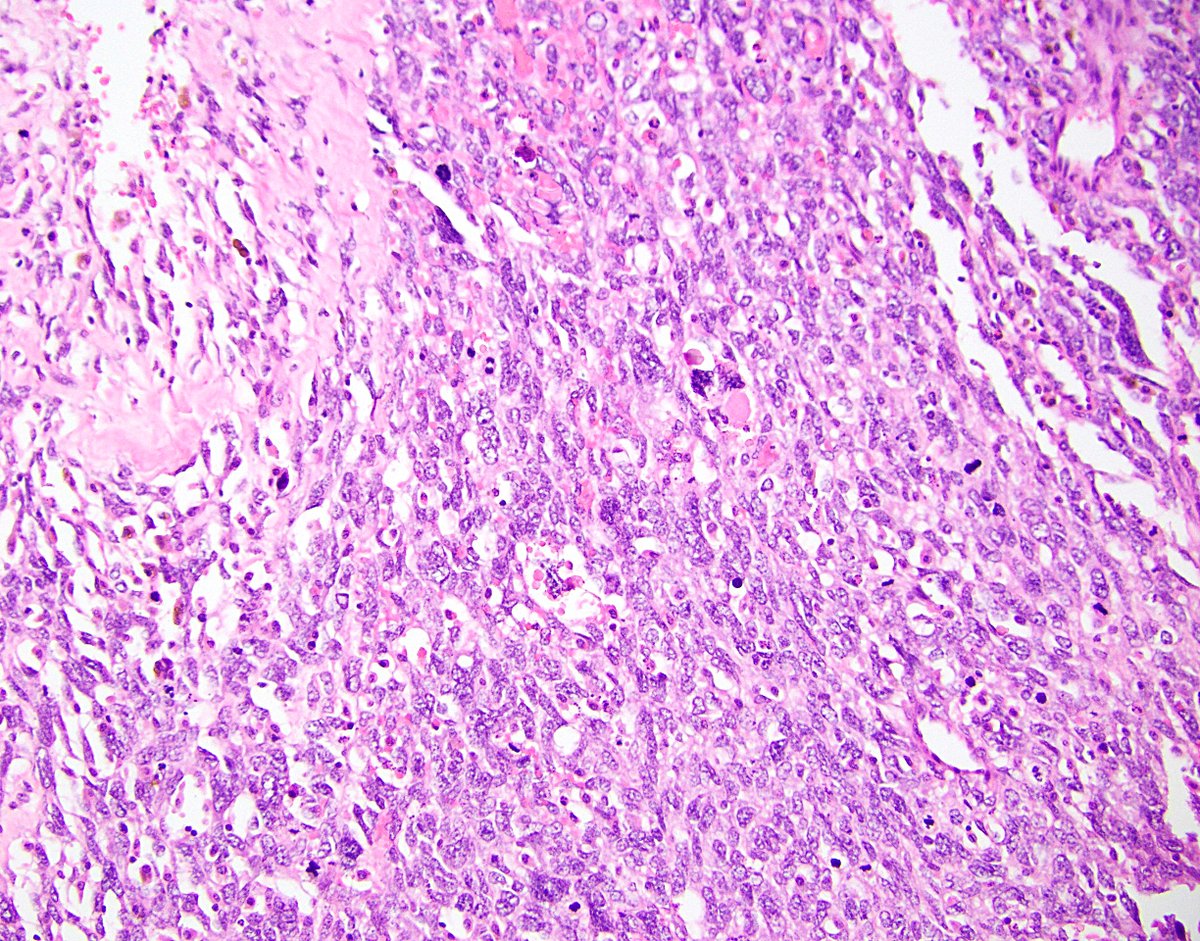
47/ Lymphoma can involve the liver, either arising or “spreading” there. True mass formation is an uncommon phenomenon, but it can happen, as with this T-cell/histiocyte-rich large-B cell lymphoma.

48/ More commonly, lymphoma appears as an atypical inflammatory infiltrate throughout the parenchyma. Examples include CLL/SLL (pic 1 – looks like viral hepatitis!) and hepatosplenic T-cell lymphoma (pic 2).


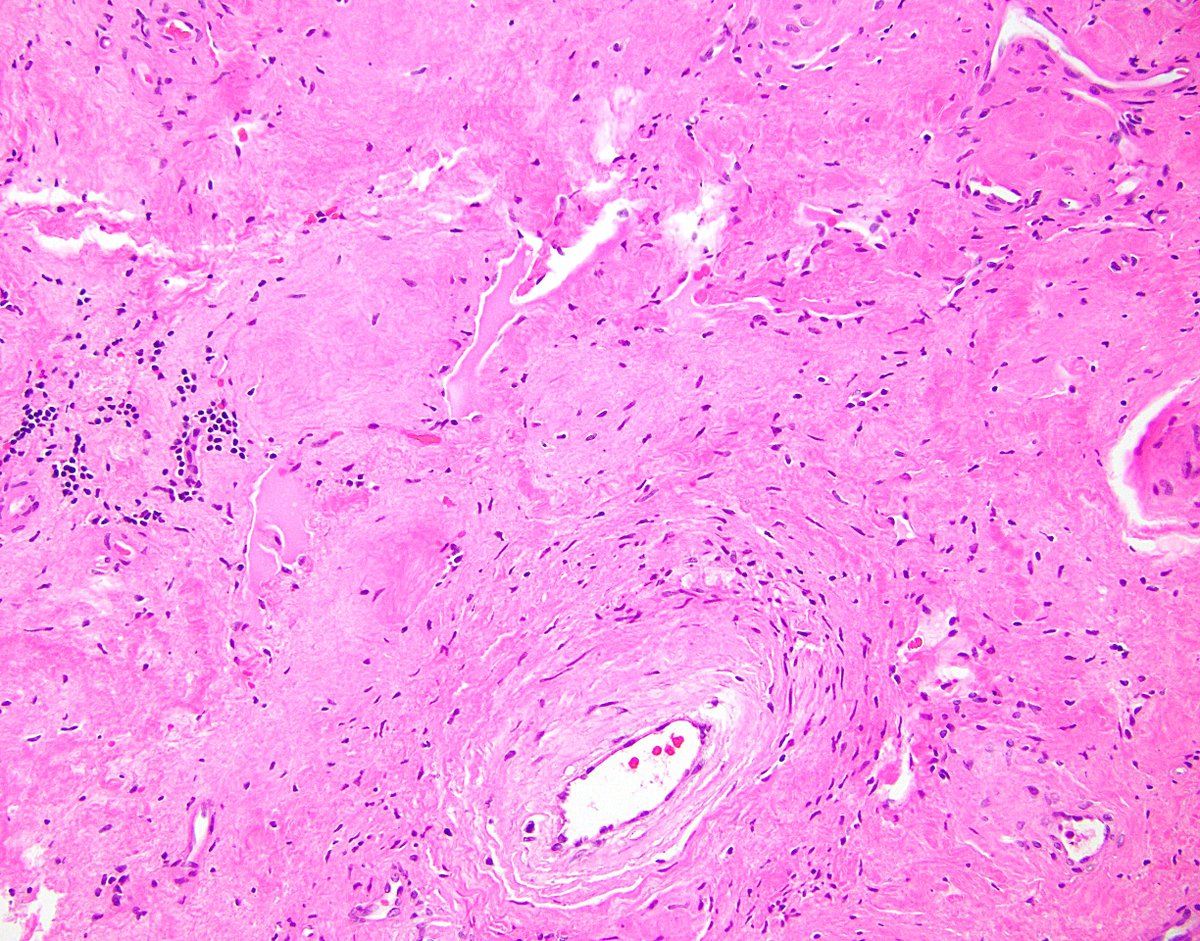
49/ We’ll end with some miscellaneous masses. Segmental atrophy is an uncommon degenerative phenomenon of the liver. The nodular elastosis stage can form a mass lesion that looks like ... well, nodular elastosis. Don’t confuse for amyloid.

50/ The liver may develop inflammatory pseudotumors from a variety of insults, including infection. Be diligent in working these up! This example showed positivity with a Treponemal immunostain, because it was caused by syphilis.


51/ Other infections can cause cystic lesions. The classic, of course, is the hydatid cyst of Echninococcus. Filled with “sand” grossly. Lamellated microscopically. Hunt for the hooklets!




52/ Some cysts are neither infectious nor neoplastic. Choledochal cyst is a simple biliary cyst arising from duct dilation. Several types based on location, including intrahepatic (pic 1 from Wikipedia). May develop dysplasia / malignancy.


53/ Much less common is ciliated hepatic foregut cyst. They are rare, probably congenital malformations with a ciliated inner lining. May also rarely progress to malignancy.

54/ Finally, I’ll end with a curveball, because there’s always weird stuff to consider. This biopsy was from a case of what ended up being diagnosed as … primary acinar cell carcinoma of the liver? bit.ly/2H1ogxI
55/ And that’s my time! I hope everyone enjoyed my second Tweetorial, which was a whopping four tweets longer than my first. I may do a third one in the future, if I can find the time. So … maybe in another year? :)

