2/11
Concept 1:
The core mechanism of respirophasic alterations of IVC diameter is its relationship with (actual, not transmural) CVP.
⬇️CVP -->⬆️venous return -->⬇️pressure within the IVC --> tendency to collapse (& vice versa).
Concept 2:
The IVC pressure-diameter relationship
Concept 1:
The core mechanism of respirophasic alterations of IVC diameter is its relationship with (actual, not transmural) CVP.
⬇️CVP -->⬆️venous return -->⬇️pressure within the IVC --> tendency to collapse (& vice versa).
Concept 2:
The IVC pressure-diameter relationship
3/11
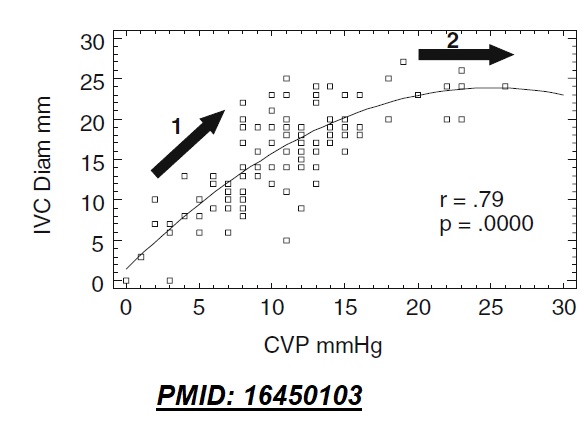
Since ΔIVC pressure is related to changes in CVP (concept 1), a direct relationship between CVP and IVC diameter exists (image)
Note that as the IVC dilates, its compliance reduces (stiffens). Hence, any further increase in IVC pressure doesn't increase its diameter.
Since ΔIVC pressure is related to changes in CVP (concept 1), a direct relationship between CVP and IVC diameter exists (image)
Note that as the IVC dilates, its compliance reduces (stiffens). Hence, any further increase in IVC pressure doesn't increase its diameter.
4/11
##IVC evaluation in a spontaneously breathing patient -
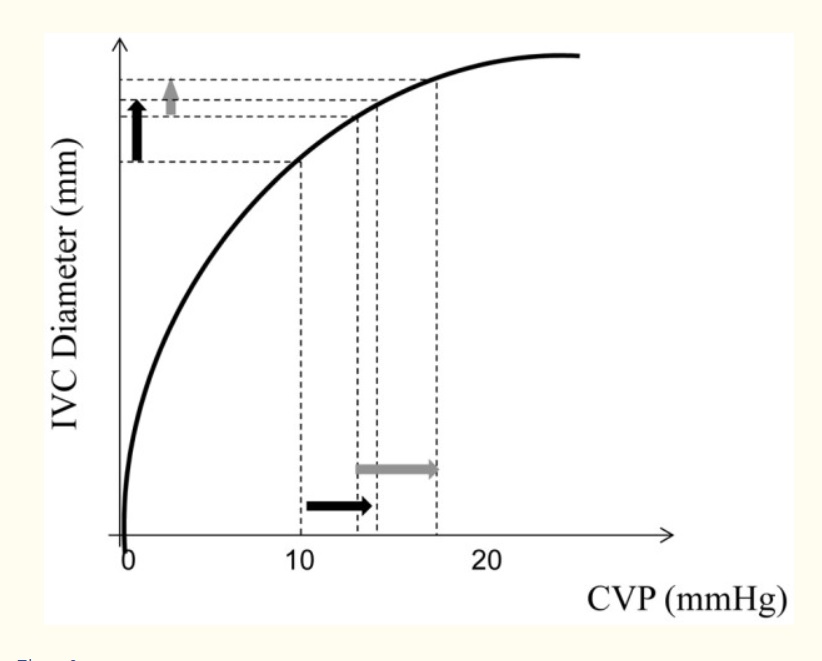
Inspiration --> ⬇️ITP --> ⬇️CVP --> ⬇️IVC diameter (IVC collapses)
Say CVP reduces by 5 mmHg upon inspiration. Note that the effect on IVC diameter (collapsibility) would be much greater if baseline CVP is lower.
##IVC evaluation in a spontaneously breathing patient -
Inspiration --> ⬇️ITP --> ⬇️CVP --> ⬇️IVC diameter (IVC collapses)
Say CVP reduces by 5 mmHg upon inspiration. Note that the effect on IVC diameter (collapsibility) would be much greater if baseline CVP is lower.
5/11
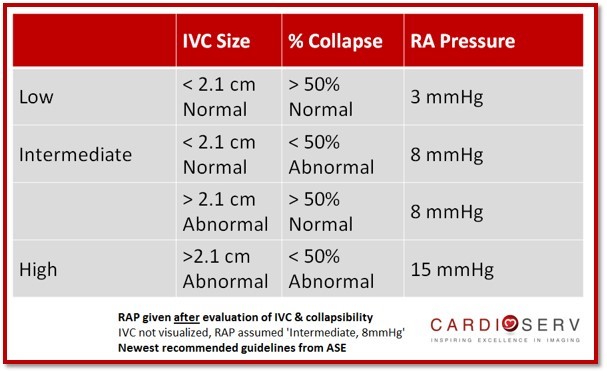
It thus makes sense that IVC collapsibility can be used to predict CVP, as has been shown.
Notably, IVC collapsibility has NOT been found to be useful predicting fluid responsiveness. Lack of standardization of inspiratory effort being one of the reasons (PMID: 27940277)
It thus makes sense that IVC collapsibility can be used to predict CVP, as has been shown.
Notably, IVC collapsibility has NOT been found to be useful predicting fluid responsiveness. Lack of standardization of inspiratory effort being one of the reasons (PMID: 27940277)
6/11
##IVC evaluation in a passive MV patient-
In passive PPV (i.e. no patient efforts e.g. paralyzed):
Inspiration --> ⬆️ITP --> ⬆️CVP --> ⬆️IVC diameter (IVC distends)
Again, the degree of IVC distension will depend on the CVP that would affect how full it is at baseline.
##IVC evaluation in a passive MV patient-
In passive PPV (i.e. no patient efforts e.g. paralyzed):
Inspiration --> ⬆️ITP --> ⬆️CVP --> ⬆️IVC diameter (IVC distends)
Again, the degree of IVC distension will depend on the CVP that would affect how full it is at baseline.
7/11
Curiously, as opposed to IVC collapsibility (in NPV), IVC distensibility (in PPV) has NOT shown good correlation with baseline CVP (but very limited data: PMID: 1466886)
However, IVC distensibility HAS shown to predict fluid responsiveness in highly standardized conditions:
Curiously, as opposed to IVC collapsibility (in NPV), IVC distensibility (in PPV) has NOT shown good correlation with baseline CVP (but very limited data: PMID: 1466886)
However, IVC distensibility HAS shown to predict fluid responsiveness in highly standardized conditions:
8/11
These include (i)Passive PPV (ii)TV - 8-12 cc/kg (iii)No cor pulmonale
A distensible IVC is interpreted as evidence of "preload reserve"
But note these are all indirect predictors of fluid responsiveness & in my mind, inferior in principle to direct predictors such as PLR
These include (i)Passive PPV (ii)TV - 8-12 cc/kg (iii)No cor pulmonale
A distensible IVC is interpreted as evidence of "preload reserve"
But note these are all indirect predictors of fluid responsiveness & in my mind, inferior in principle to direct predictors such as PLR
9/11
##IVC evaluation in patient-triggered PPV -
This scenario is much more common and rather complex. Patients often have alternating patient-triggered and machine-triggered breaths..
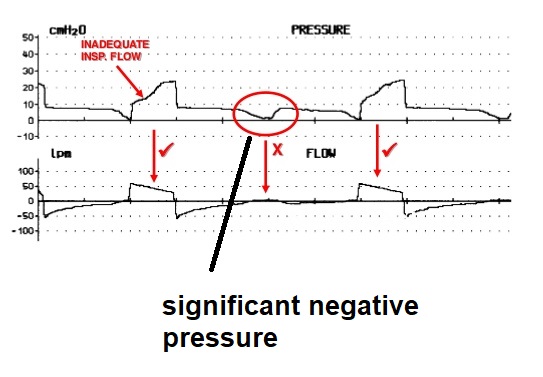
In a patient-triggered breath, there is an initial dip in ITP as the patient triggers.
##IVC evaluation in patient-triggered PPV -
This scenario is much more common and rather complex. Patients often have alternating patient-triggered and machine-triggered breaths..
In a patient-triggered breath, there is an initial dip in ITP as the patient triggers.
10/11
This negative dip may be rather pronounced if the respiratory drive is high (e.g. flow starvation in volume control). This may cause IVC collapsibility per prior discussion.
However, I would offer caution in using this for CVP estimation as other factors may affect the IVC
This negative dip may be rather pronounced if the respiratory drive is high (e.g. flow starvation in volume control). This may cause IVC collapsibility per prior discussion.
However, I would offer caution in using this for CVP estimation as other factors may affect the IVC
11/11
This includes⬆️abdominal pressure with PPV (see Jon Emile's articles on PulmCCM)
Summary -
-NPV: IVC collapsibility is most helpful in estimating CVP
-Passive PPV: IVC distensibility can predict FR
-Patient-triggered PPV - IVC may collapse but use caution in interpreting.
This includes⬆️abdominal pressure with PPV (see Jon Emile's articles on PulmCCM)
Summary -
-NPV: IVC collapsibility is most helpful in estimating CVP
-Passive PPV: IVC distensibility can predict FR
-Patient-triggered PPV - IVC may collapse but use caution in interpreting.