
🖍️ & 🥃 Episode 2 : TESTING (part 1)
Let’s talk about testing!
To start, there are 2 types of testing:
1. Viral tests: used to detect ACTIVE infection
2. Serology (antibody) tests - to detect PREVIOUS infection
Today we talk about VIRAL tests, & serology tomorrow.
Let's go!
Let’s talk about testing!
To start, there are 2 types of testing:
1. Viral tests: used to detect ACTIVE infection
2. Serology (antibody) tests - to detect PREVIOUS infection
Today we talk about VIRAL tests, & serology tomorrow.
Let's go!
Viral tests help diagnose ACTIVE infection, NOT previous infection.
We test to better understand:
Who is sick with COVID?
How the disease is spreading?
What % of those infected survive?
What % of cases are asymptomatic (capable of spreading the virus even with no symptoms)?
We test to better understand:
Who is sick with COVID?
How the disease is spreading?
What % of those infected survive?
What % of cases are asymptomatic (capable of spreading the virus even with no symptoms)?
WHO SHOULD BE TESTED?
The @CDCgov has recommendations on who should be tested, but guidance is currently led by local & state health departments.
The reality is that even with expanded testing, not everyone who is experiencing symptoms of COVID19 will be able to access testing.
The @CDCgov has recommendations on who should be tested, but guidance is currently led by local & state health departments.
The reality is that even with expanded testing, not everyone who is experiencing symptoms of COVID19 will be able to access testing.
Due to these limitations in testing, there is a priority on hospitalized patients, healthcare/ essential workers, and those in long term care facilities.
The best place to look for testing sites is your local or state health department website.
Or here: bit.ly/2zFwScQ
The best place to look for testing sites is your local or state health department website.
Or here: bit.ly/2zFwScQ
DIAGNOSING ACTIVE INFECTIONS
To detect ACTIVE infection with SARS-CoV-2 (the virus that causes COVID19), we primarily use a test called RT-PCR.
First we'll talk about RT-PCR, and then the important difference between what this test detects & what actually causes infection!
To detect ACTIVE infection with SARS-CoV-2 (the virus that causes COVID19), we primarily use a test called RT-PCR.
First we'll talk about RT-PCR, and then the important difference between what this test detects & what actually causes infection!
RT-PCR
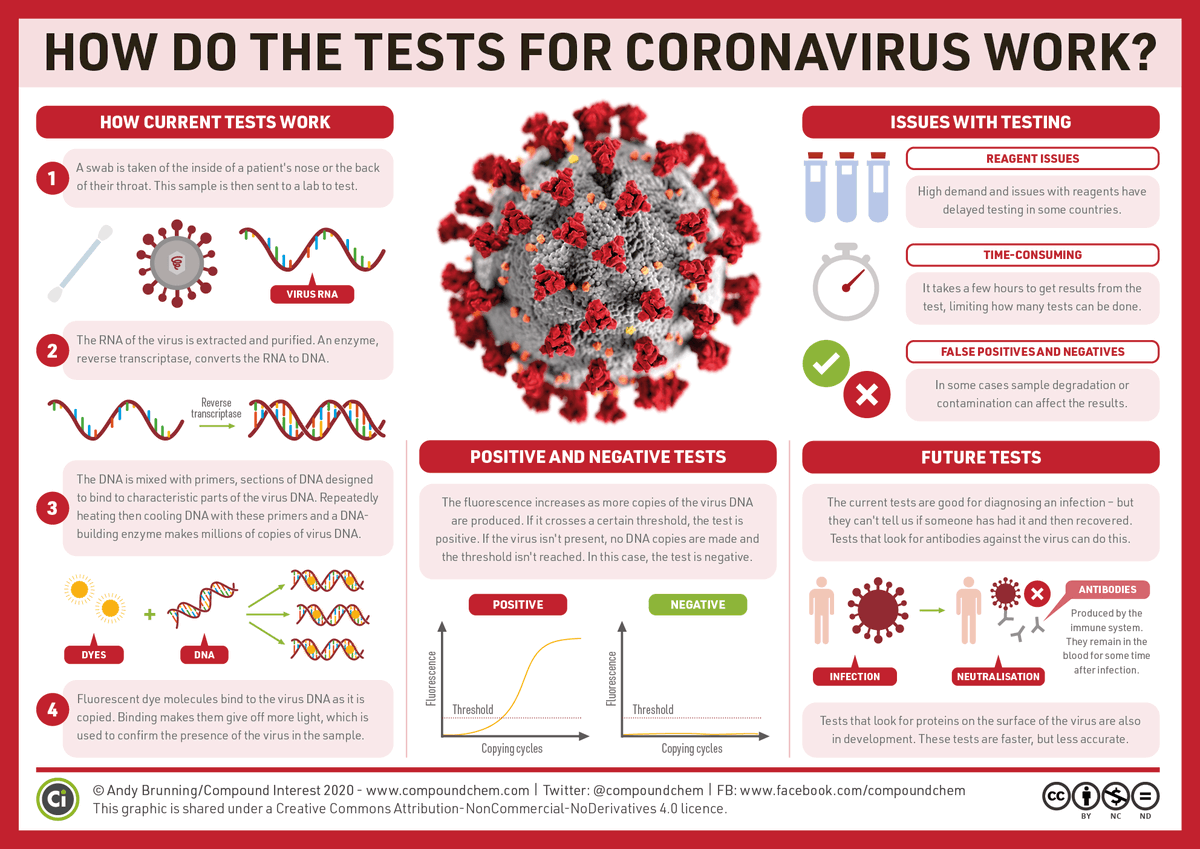
So what is RT-PCR? It's short for real-time, reverse transcriptase-polymerase chain reaction. It takes viral genetic material (RNA), turns it into DNA, and makes billions of copies of it until it reaches a set threshold for detection.
Great graphic from @compoundchem
So what is RT-PCR? It's short for real-time, reverse transcriptase-polymerase chain reaction. It takes viral genetic material (RNA), turns it into DNA, and makes billions of copies of it until it reaches a set threshold for detection.
Great graphic from @compoundchem
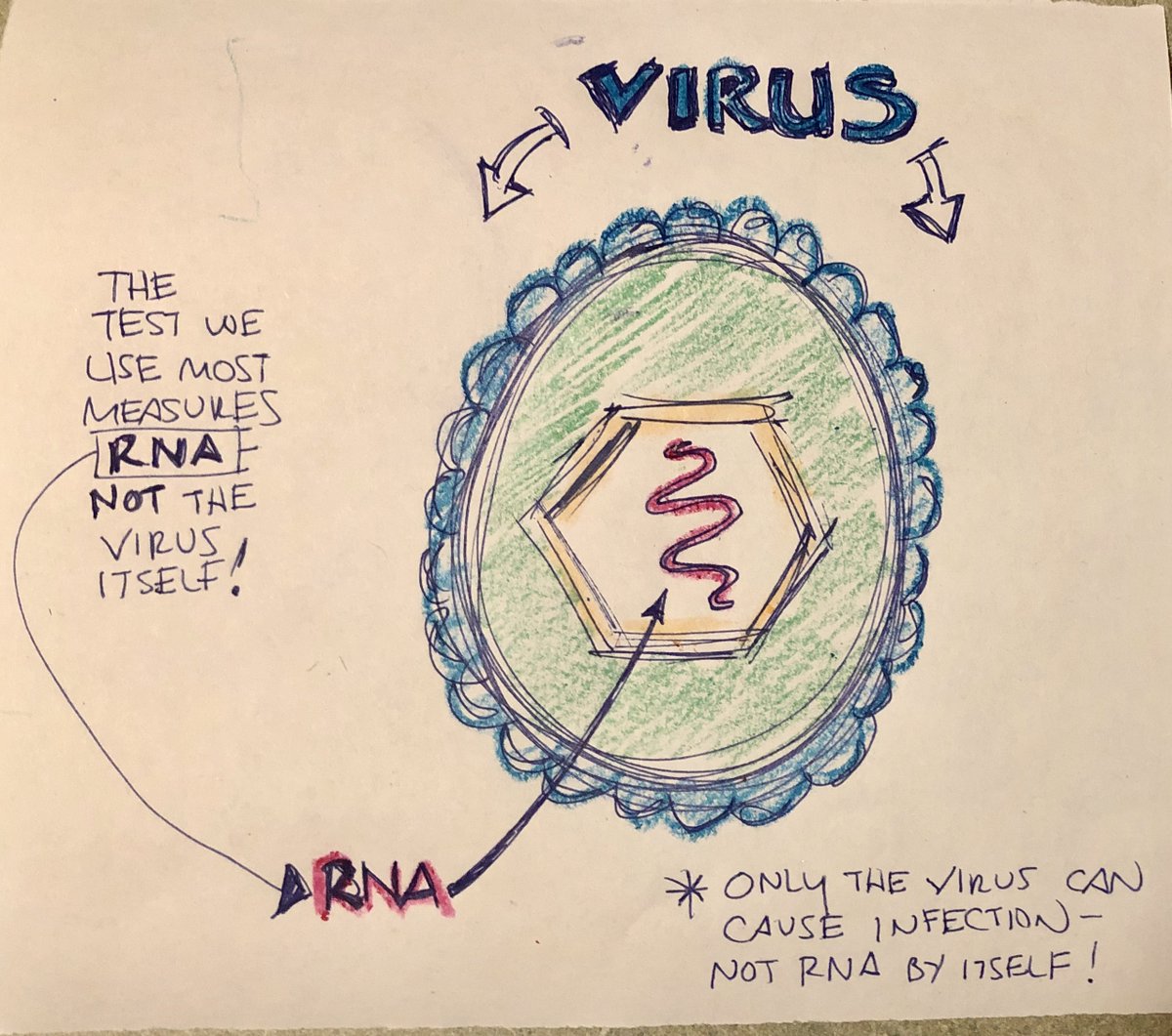
RT-PCR detects RNA only - NOT the actual virus!
RNA alone doesn’t infect you - ONLY if carried by a virus.
So if you test +, it only means the test found RNA. It doesn't say anything about infectious virus!
And you can shed leftover RNA fragments without being infectious!
RNA alone doesn’t infect you - ONLY if carried by a virus.
So if you test +, it only means the test found RNA. It doesn't say anything about infectious virus!
And you can shed leftover RNA fragments without being infectious!
SO A POSITIVE TEST DOESN’T ALWAY MEAN I HAVE COVID?
A positive test means RNA was detected is in your system.
And RT-PCR has been positive on samples from people weeks after recovery.
But we suspect that these likely represent leftover fragments - not infectious virus itself!
A positive test means RNA was detected is in your system.
And RT-PCR has been positive on samples from people weeks after recovery.
But we suspect that these likely represent leftover fragments - not infectious virus itself!
WHAT DOES TESTING INVOLVE?
For RT-PCR, we need a nasopharyngeal sample.
You'll get a specialized Q-tip swab jammed DEEP into your nose!
It's not fun - but it has to be a good sample or the test might not give the right result.
This swab is put into a solution & sent to a lab.
For RT-PCR, we need a nasopharyngeal sample.
You'll get a specialized Q-tip swab jammed DEEP into your nose!
It's not fun - but it has to be a good sample or the test might not give the right result.
This swab is put into a solution & sent to a lab.

TEST PERFORMANCE:
Just like everything in life, viral tests for COVID19 aren’t perfect. They depend a lot on certain things like:
Good specimen collection with the swab?
Did the lab use the right reagents?
Plus all tests have their own inherent issues and limitations.
Just like everything in life, viral tests for COVID19 aren’t perfect. They depend a lot on certain things like:
Good specimen collection with the swab?
Did the lab use the right reagents?
Plus all tests have their own inherent issues and limitations.
These inherent qualities of the tests themselves are called SENSITIVITY & SPECIFICITY.
No test is 100%.
Even if you DO have COVID19, sometimes the test will be negative.
Or even if you DON’T have COVID19, sometimes you’ll still test positive! This is important!
No test is 100%.
Even if you DO have COVID19, sometimes the test will be negative.
Or even if you DON’T have COVID19, sometimes you’ll still test positive! This is important!
FALSE NEGATIVE AND FALSE POSITIVE:
SENSITIVITY is the probability a sample will be positive if the patient is ACTUALLY sick (it correctly says you have the disease when you do!).
So if 100 patients with COVID are tested and 95 test positive, the test is 95% sensitive.
SENSITIVITY is the probability a sample will be positive if the patient is ACTUALLY sick (it correctly says you have the disease when you do!).
So if 100 patients with COVID are tested and 95 test positive, the test is 95% sensitive.

But there are reasons why someone might be a FALSE NEGATIVE (meaning the test is negative EVEN THOUGH they HAVE the disease!)
Sample wasn’t collected well, problem with the test, low amount of virus present, etc…
So we'd tell people who have COVID that they don’t. Big problem!
Sample wasn’t collected well, problem with the test, low amount of virus present, etc…
So we'd tell people who have COVID that they don’t. Big problem!
On the other hand, SPECIFICITY is the probability a sample will test negative if the patient does NOT have the disease (‘ruling out disease’).
However, sometimes people WITHOUT the disease CAN test positive (due to lab contamination, swab mixup, etc)! These are FALSE POSITIVES.
However, sometimes people WITHOUT the disease CAN test positive (due to lab contamination, swab mixup, etc)! These are FALSE POSITIVES.

Most tests do NOT have 100% sensitivity & specificity. It’s often a trade off.
The result is that some people who HAVE COVID are told they don’t. And some who don’t have COVID are told they do!
This'll be important when we talk about negative - positive - negative tests later.
The result is that some people who HAVE COVID are told they don’t. And some who don’t have COVID are told they do!
This'll be important when we talk about negative - positive - negative tests later.
HOW MANY TESTS HAVE WE DONE?
To date, we’ve done ~6.8 million tests in the USA. Just over 1.1 million have been positive (~16.5%).
And the past week, we’ve averaged about 231,400 tests per day.
That number has increased in the past few weeks, which is good.
But…
To date, we’ve done ~6.8 million tests in the USA. Just over 1.1 million have been positive (~16.5%).
And the past week, we’ve averaged about 231,400 tests per day.
That number has increased in the past few weeks, which is good.
But…

HOW MANY TESTS DO WE NEED?
There are various estimates of how many tests we need to be doing to tackle COVID - but everyone agrees that we need WAY more tests being done every day!
One Harvard study says at least 500k/day. bit.ly/3d9o65w
Others say MILLIONS per day!
There are various estimates of how many tests we need to be doing to tackle COVID - but everyone agrees that we need WAY more tests being done every day!
One Harvard study says at least 500k/day. bit.ly/3d9o65w
Others say MILLIONS per day!
Why so many?
We want the proportion of positive tests to be as low as possible, ideally <10%.
If it’s any higher, it means we aren’t testing enough. Which means there are people with COVID in the community who can be spreading the disease.
Currently in the US that # is ~16.5%
We want the proportion of positive tests to be as low as possible, ideally <10%.
If it’s any higher, it means we aren’t testing enough. Which means there are people with COVID in the community who can be spreading the disease.
Currently in the US that # is ~16.5%

CHALLENGES OF RAMPING UP TESTING:
In addition to just MAKING more tests, theres a lot more we need to DO more tests.
You need healthcare workers to do the tests, swabs, and personal protective equipment.
Many of these were in short supply, slowing the increase in testing.
In addition to just MAKING more tests, theres a lot more we need to DO more tests.
You need healthcare workers to do the tests, swabs, and personal protective equipment.
Many of these were in short supply, slowing the increase in testing.
WHAT ABOUT + then - then +?
There have been reports of people testing +, then testing -, then testing + again.
So does that mean you can have COVID, get better, and get sick right away again?
Probably not.
This may reflect limitations of the tests - remember false negatives!
There have been reports of people testing +, then testing -, then testing + again.
So does that mean you can have COVID, get better, and get sick right away again?
Probably not.
This may reflect limitations of the tests - remember false negatives!
ARE THERE OTHER WAYS TO DETECT ACTIVE COVID?
Yup! There are molecular assays, protein tests, and point-of-care tests all under development right now.
There’s even a FDA approved home test.
And CT scans can help diagnose COVID, but it’s not as sensitive or practical as others.
Yup! There are molecular assays, protein tests, and point-of-care tests all under development right now.
There’s even a FDA approved home test.
And CT scans can help diagnose COVID, but it’s not as sensitive or practical as others.
ANTIGEN TESTS:
Soon you’ll hear more about antigen tests.
Instead of looking for genetic material like RT-PCR, these tests look for proteins on the outside of the virus.
They can be done MUCH faster, but the results aren’t nearly as accurate.
For now, RT-PCR is king! 🧪👑
Soon you’ll hear more about antigen tests.
Instead of looking for genetic material like RT-PCR, these tests look for proteins on the outside of the virus.
They can be done MUCH faster, but the results aren’t nearly as accurate.
For now, RT-PCR is king! 🧪👑
Thanks to everyone who asked questions about testing, including @offgridteacher @jontyglaser @mitote83.
For our next episode, we’ll tackle serology (antibody) testing.
This thread (and future ones) + all supporting articles & research can be found at: bit.ly/3bRycHQ
For our next episode, we’ll tackle serology (antibody) testing.
This thread (and future ones) + all supporting articles & research can be found at: bit.ly/3bRycHQ
Thanks to @TylerWen & @saurabhsudesh for helping put this together!
And as a reminder, the goal is to share something like this every night for a week at ~9pm to address big questions around testing, treatments, vaccines, pathophysiology and more!
Powered by 🖍️ & 🥃.
Be safe!
And as a reminder, the goal is to share something like this every night for a week at ~9pm to address big questions around testing, treatments, vaccines, pathophysiology and more!
Powered by 🖍️ & 🥃.
Be safe!


