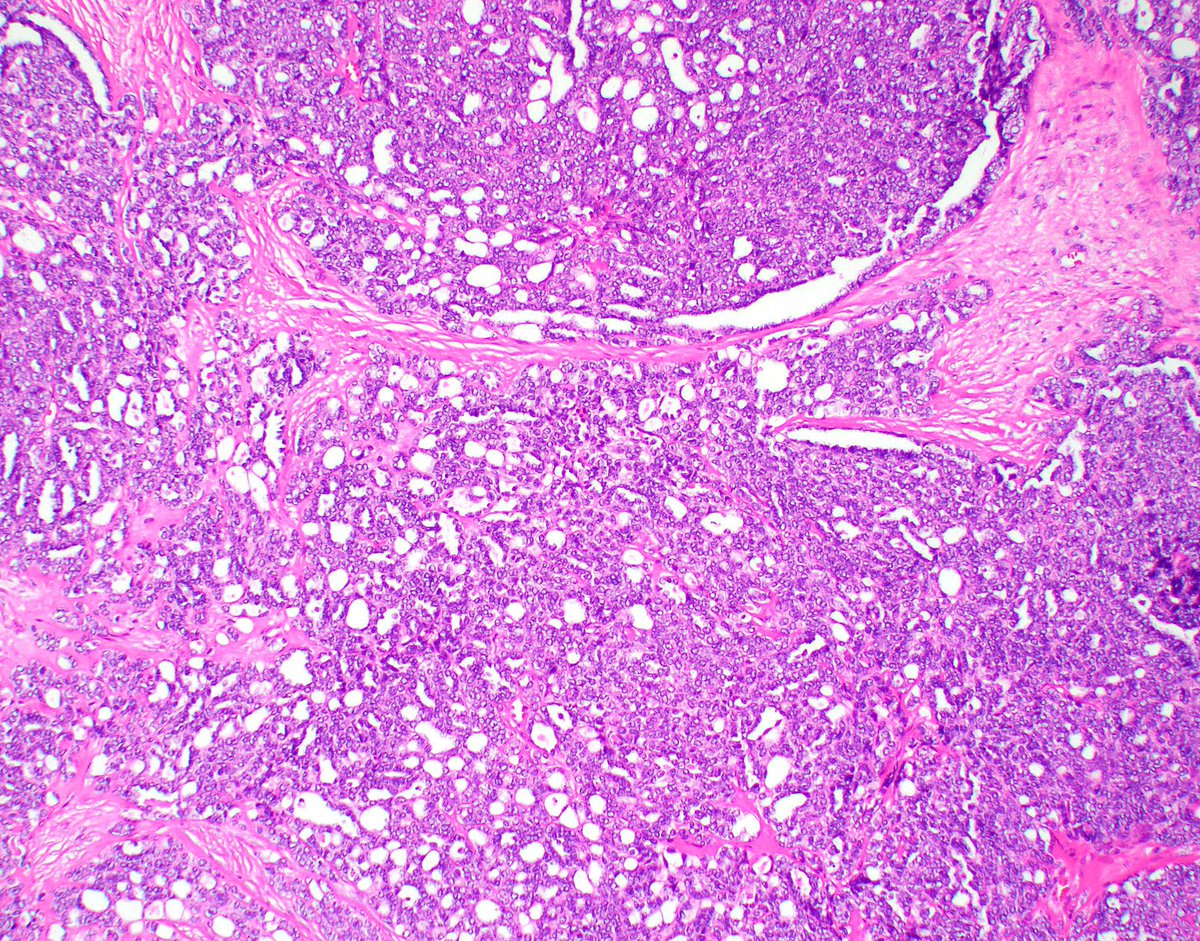
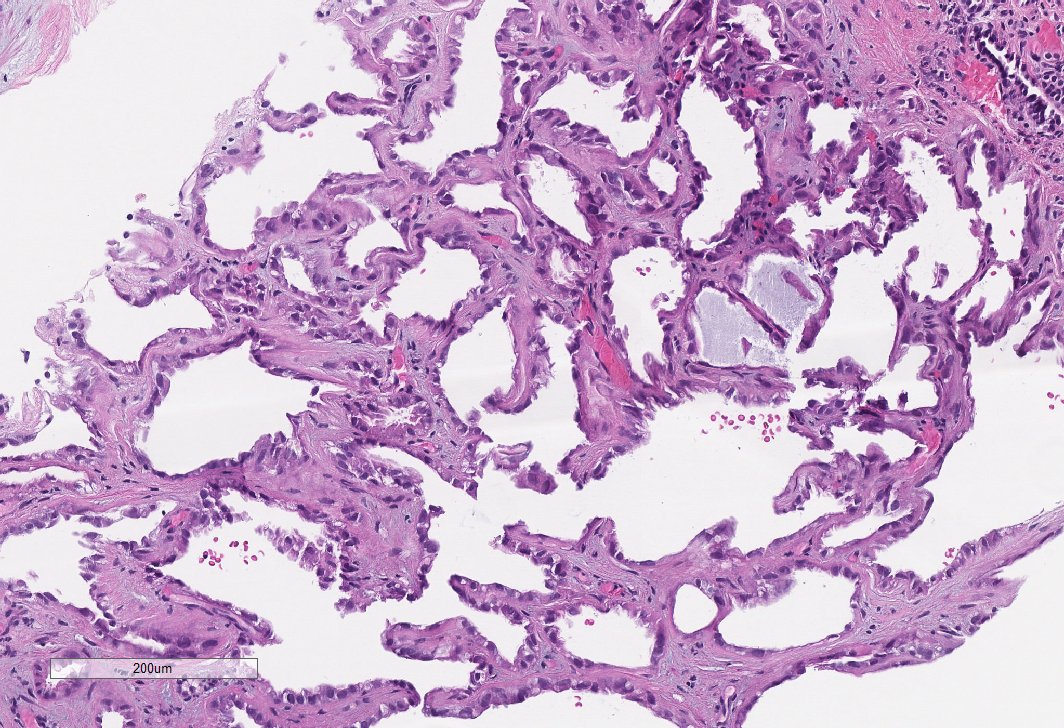
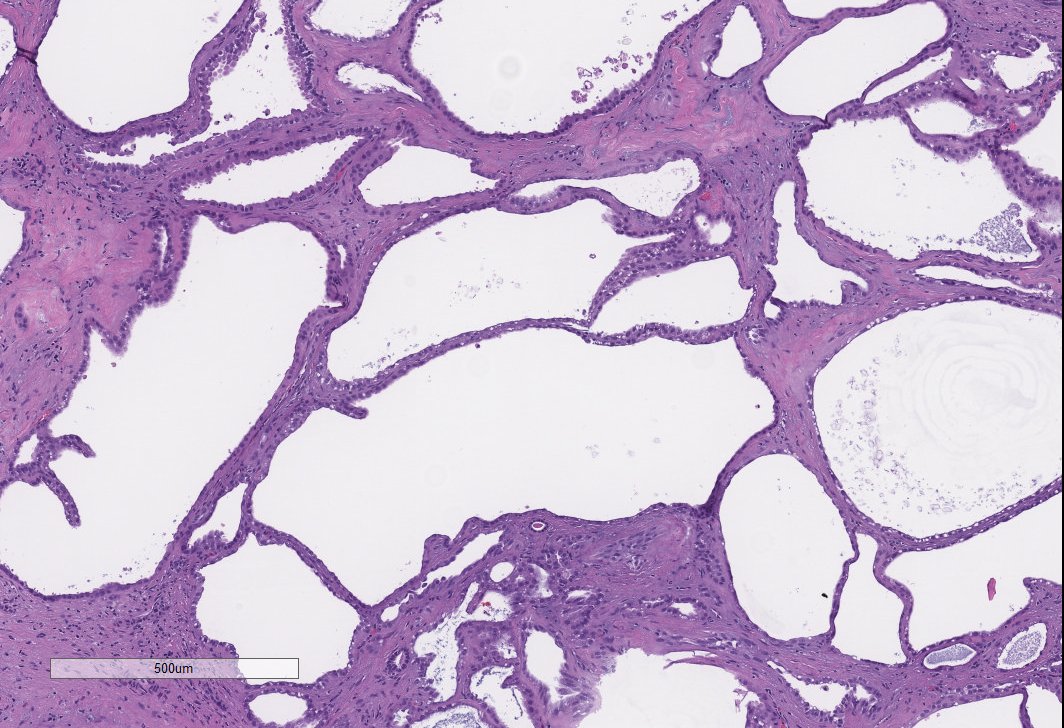
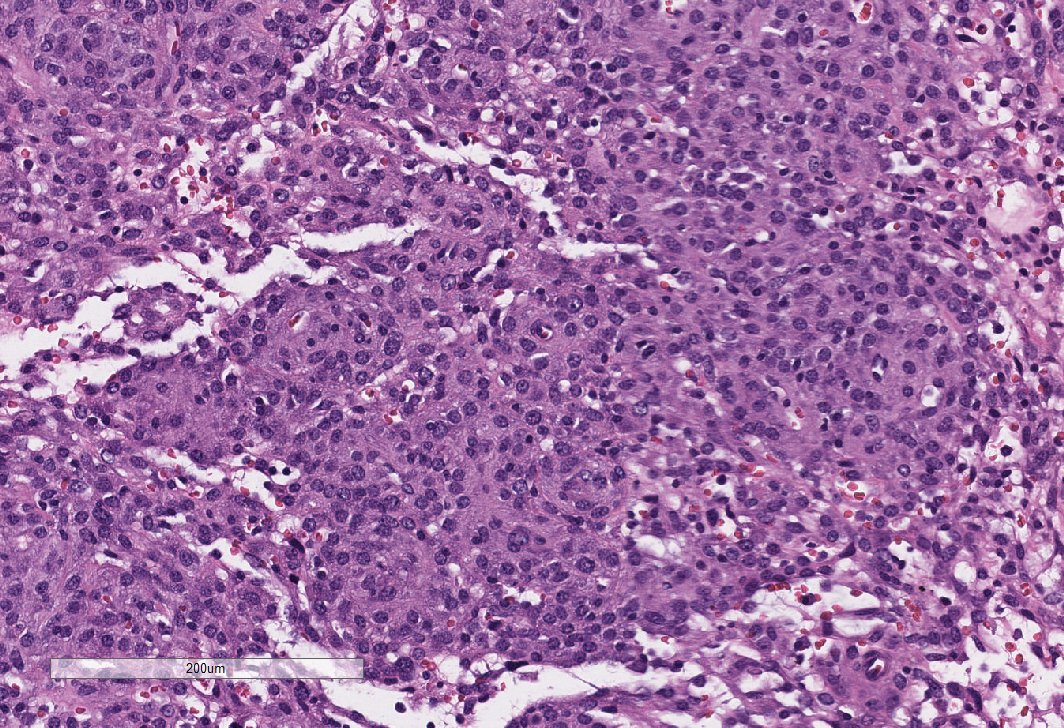
Renal tumor in a 19 year old. Stains and diagnosis 👇 #GUpath 


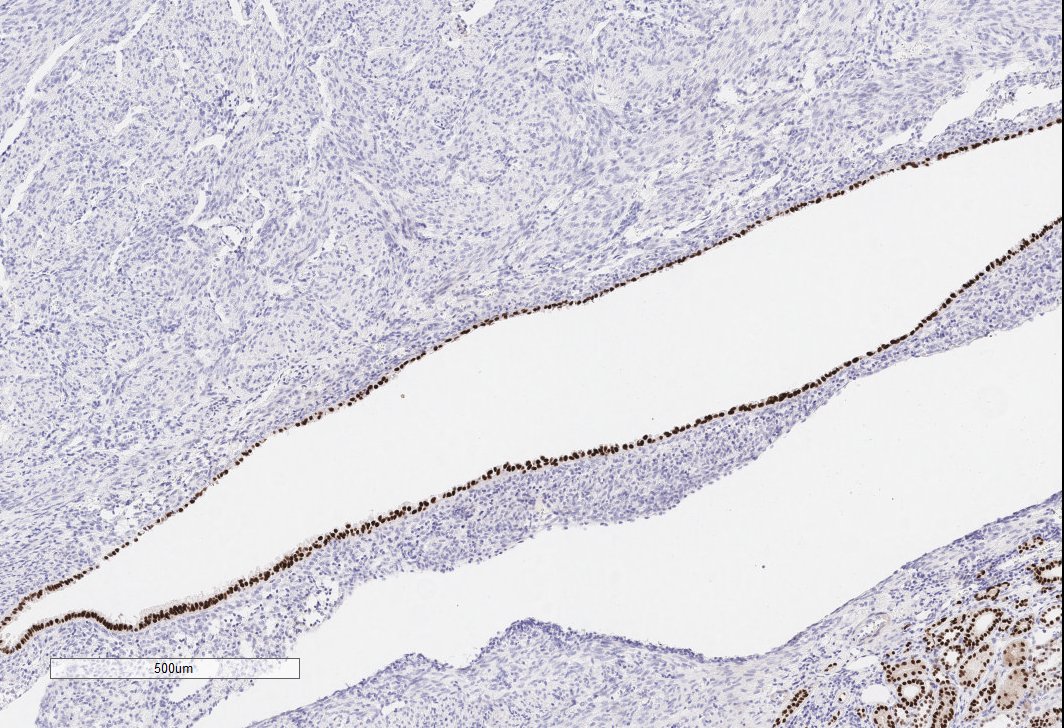
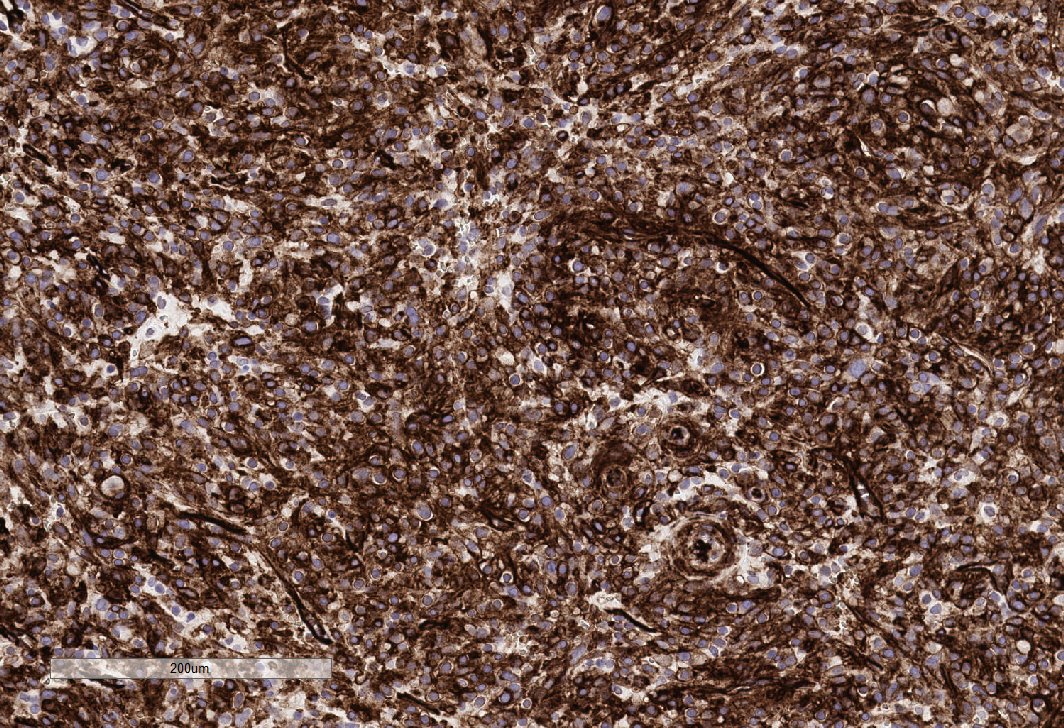
CD117 and Synaptophysin (pictures) +. PAX8 -

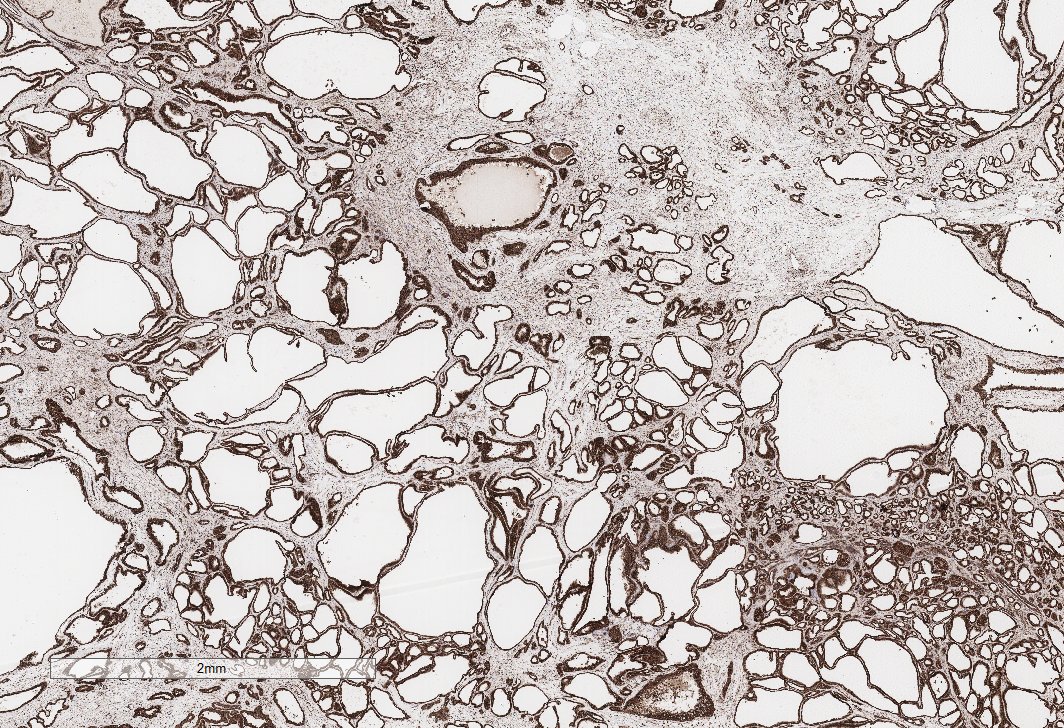
CD34+ (pic) keratin -
Diagnosis: Juxtaglomerular cell tumor. #GUpath
Often in young patients and in the D/D of oncocytic renal tumors. Always a good idea to run a keratin and a PAX8 when in doubt. Don't be fooled by the CD117 staining.
Often in young patients and in the D/D of oncocytic renal tumors. Always a good idea to run a keratin and a PAX8 when in doubt. Don't be fooled by the CD117 staining.
• • •
Missing some Tweet in this thread? You can try to
force a refresh