#Cardiotwitter. Continuing the series on time intervals, I’ll now use some time on the ejection period. It’s not as simple as it may seem at first glance, and there is a lot going on. 

1/ Comparing a tension length diagram of an isotonic/isometric twitch, and a pressure/volume (Wiggers)diagram. I've added the division of pre ejection into protosystole and IVC from previous threads.

2/ The ejection period is not isotonic, as pressure increases and then decreases, and the myocardial tension must follow a similar course. Thus the tension increase is only during the first part of ejection, and then tension decline so last part of ejection is relaxation
3/ With conventional pressure/flow recordings, the peak pressure / tension is around mid ejection, but looking at flow, peak flow through aortic ostium is much earlier. Peak flow must mean peak rate of volume decrease, and occurs early during ejection.

4/ Flow velocity (m/s) is a nice proxy for flow (l/min), as long ar the postal area is constant., and peak flow velocity is likewise an early event during ejection.

5/ Annular velocity is the peak rate of shortening, which again is a proxy for the rate of volume decrease. Peak annular velocity is likewise an early event during ejection, and peak flow and peak shortening velocity are closely related.


6/ As we see, annular velocity is equivalent to the inverse of strain rate of the wall ncbi.nlm.nih.gov/pubmed/32154940,
annular displacement is equivalent to the inverse of strain ncbi.nlm.nih.gov/pubmed/29399886, so all of these are related
annular displacement is equivalent to the inverse of strain ncbi.nlm.nih.gov/pubmed/29399886, so all of these are related

7/ And, there is a nice correspondence between volume curve and strain curve, fiber shortening corresponds to volume reduction, so SV/EF and GLS are closely related.

8/ We know that both SV and EF, and thus MAPSE and GLS are afterload dependent, shortening is tension vs load.

9/ The rate of tension development during isovolumic shortening is not afterload dependent, as discussed before. But the rate of shortening (which occurs during ejection) is afterload dependent, so the peak velocities will be as well.

10/ Peak flow/velocity/shortening rate is thus earlier than peak tension/pressure, possibly due to pressure (load) increase during early ejection; thus, peak velocity is a function not only of contraction velocity, but of timing of the peak.

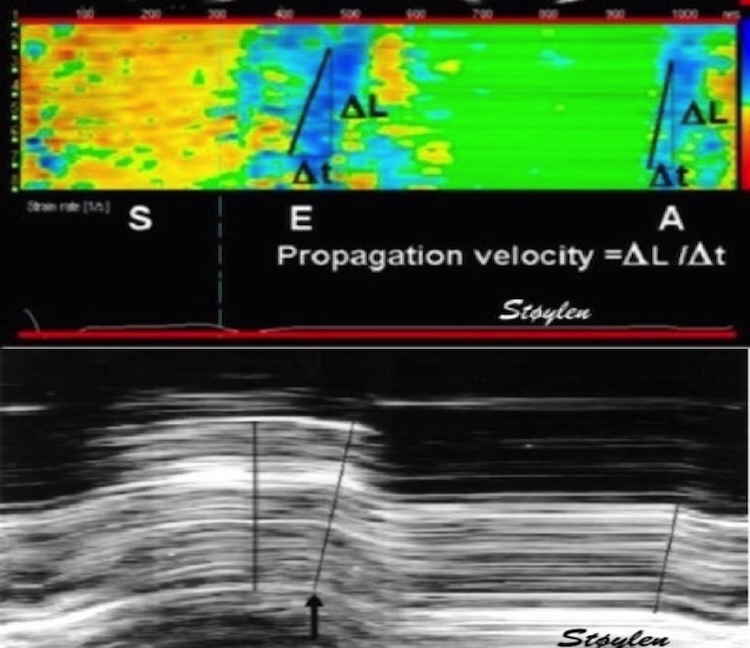
11/ Timing of peak is thus afterload dependent by the increase in ejection pressure, which is a function of not only resistance, but also of aortic stiffness, which again is of both compliance, and pressure augmentation index (pulse propagation velocity).

unroll
@threadreaderapp
@threadreaderapp
• • •
Missing some Tweet in this thread? You can try to
force a refresh