
Cardiovascular physiology. Academic tweets now also on bluesky. Staying on X for other contents.
 2/ AV-plane motion exerts opposite effects on the ventricles and atria: LV shortening vs Atrial elongation in systole, LV elongation and atrial expansion during early and late LV diastole. Thus, both LV and LA strain are inseparable from AV-plane motion.
2/ AV-plane motion exerts opposite effects on the ventricles and atria: LV shortening vs Atrial elongation in systole, LV elongation and atrial expansion during early and late LV diastole. Thus, both LV and LA strain are inseparable from AV-plane motion. 
 The full picture is far more complex, the typical version of the Wiggers diagram as shown here, do not show the effects of inertia of blood, the knowledge from newer physiological studies with high-fidelity catheters, nor from Doppler and TDI. Let’s look at what’s missing.
The full picture is far more complex, the typical version of the Wiggers diagram as shown here, do not show the effects of inertia of blood, the knowledge from newer physiological studies with high-fidelity catheters, nor from Doppler and TDI. Let’s look at what’s missing.
 2/ It was shown in the early 60ies that the pressure gradient from LV to Aorta was positive only during early ejection, and then negative during most of ejection. Pressure crossover occurred earlier than peak pressure. pubmed.ncbi.nlm.nih.gov/13915694/
2/ It was shown in the early 60ies that the pressure gradient from LV to Aorta was positive only during early ejection, and then negative during most of ejection. Pressure crossover occurred earlier than peak pressure. pubmed.ncbi.nlm.nih.gov/13915694/

 2/ This means, both phases consist of a wall elongation wave, generating an AV-plane motion away from the apex. So what are the differences?
2/ This means, both phases consist of a wall elongation wave, generating an AV-plane motion away from the apex. So what are the differences? 

 2/ Myoccyte relaxation actually starts during ejection at the time of peak pressure, the decreasing pressure during ejection shows decreasing myocyte tension. pubmed.ncbi.nlm.nih.gov/6227428/
2/ Myoccyte relaxation actually starts during ejection at the time of peak pressure, the decreasing pressure during ejection shows decreasing myocyte tension. pubmed.ncbi.nlm.nih.gov/6227428/
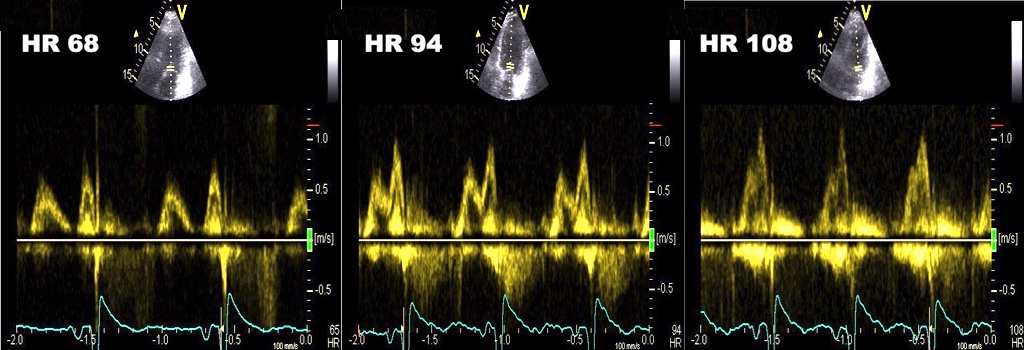 2/ also, it should be well known that this occurs because the diastole shortens more with high HR than systole. But why?
2/ also, it should be well known that this occurs because the diastole shortens more with high HR than systole. But why?
 2/ Values are age dependent, and in fact mean of 2 walls was 8.37 cm/s, and of four walls 8.4 cm/s, the difference was statistically significant, but totally un interesting as lower measurement limit of pwTDI is 0.1 cm/s. folk.ntnu.no/stoylen/strain…
2/ Values are age dependent, and in fact mean of 2 walls was 8.37 cm/s, and of four walls 8.4 cm/s, the difference was statistically significant, but totally un interesting as lower measurement limit of pwTDI is 0.1 cm/s. folk.ntnu.no/stoylen/strain…







 2/ But what does these measures signify physiologically? Taking a look at the atrial and ventricular strain curves from the same ventricle is interesting. As we see, the two sets of curves are reciprocal.
2/ But what does these measures signify physiologically? Taking a look at the atrial and ventricular strain curves from the same ventricle is interesting. As we see, the two sets of curves are reciprocal. 

