
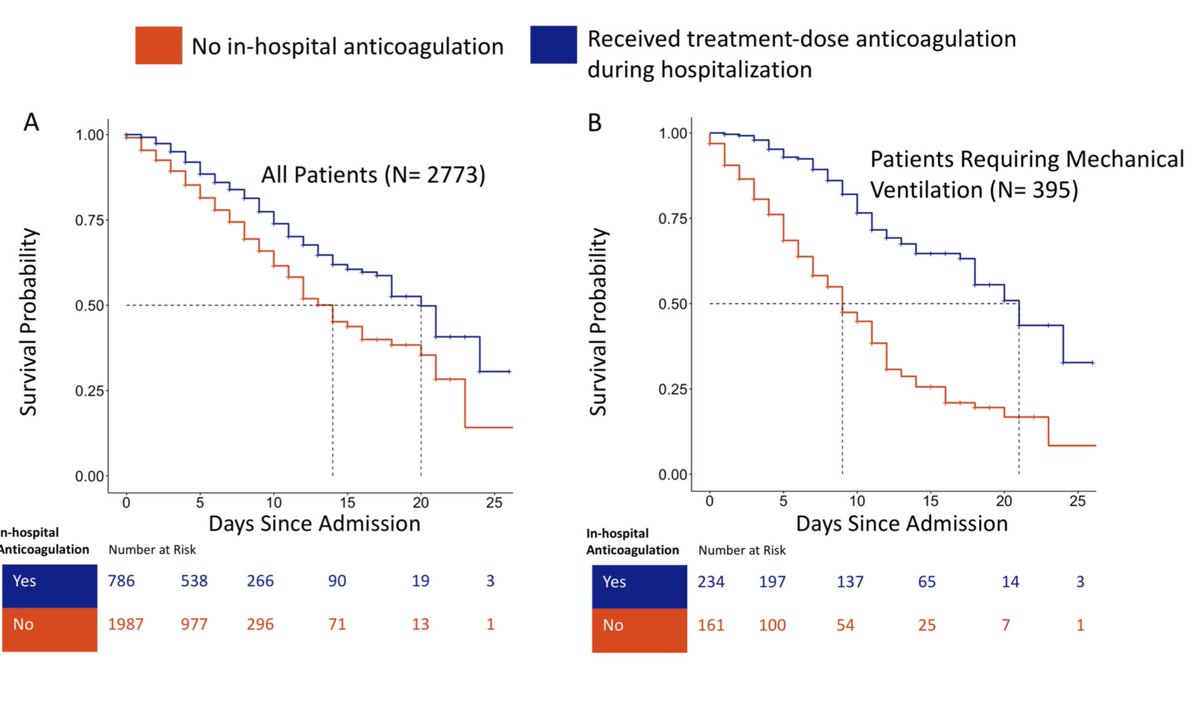
Observational study of n=786 #COVID pt who received treatment dose #anticoagulation (AC) vs n=1987 who did not. AC associated w/ decreased mortality, particularly in intubated patients (29.1% vs 62.7%).
Non-randomized & sparse on details but promising.
➡️bit.ly/35DX97f
Non-randomized & sparse on details but promising.
➡️bit.ly/35DX97f

Before getting too excited about this *observational* study remember two key points:
1. Mount Sinai made therapeutic AC their standard of care for ICU pt w/ COVID. Therefore among intubated pt comparing AC vs not is really just comparing AC to people where AC was contraindicated.
1. Mount Sinai made therapeutic AC their standard of care for ICU pt w/ COVID. Therefore among intubated pt comparing AC vs not is really just comparing AC to people where AC was contraindicated.
2. As @DrToddLee points out, this is an example of immortal time bias. A median of 2 days (range 0-5) elapsed b/w admit and beginning AC & much mortality occurs in the first 2 ICU days; thus early mortality is disproportionately counted in non-AC group ➡️bit.ly/3bbAa4N
• • •
Missing some Tweet in this thread? You can try to
force a refresh
































