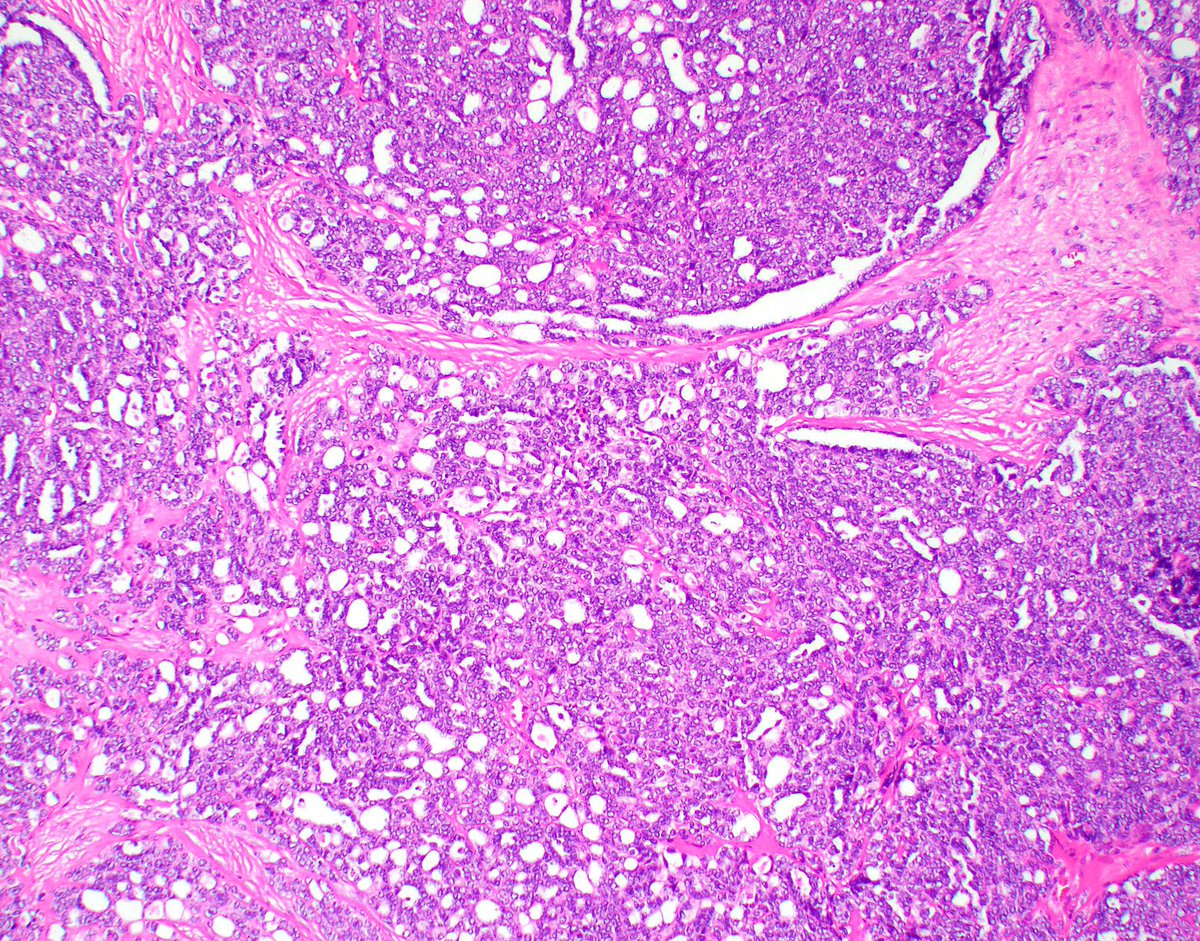
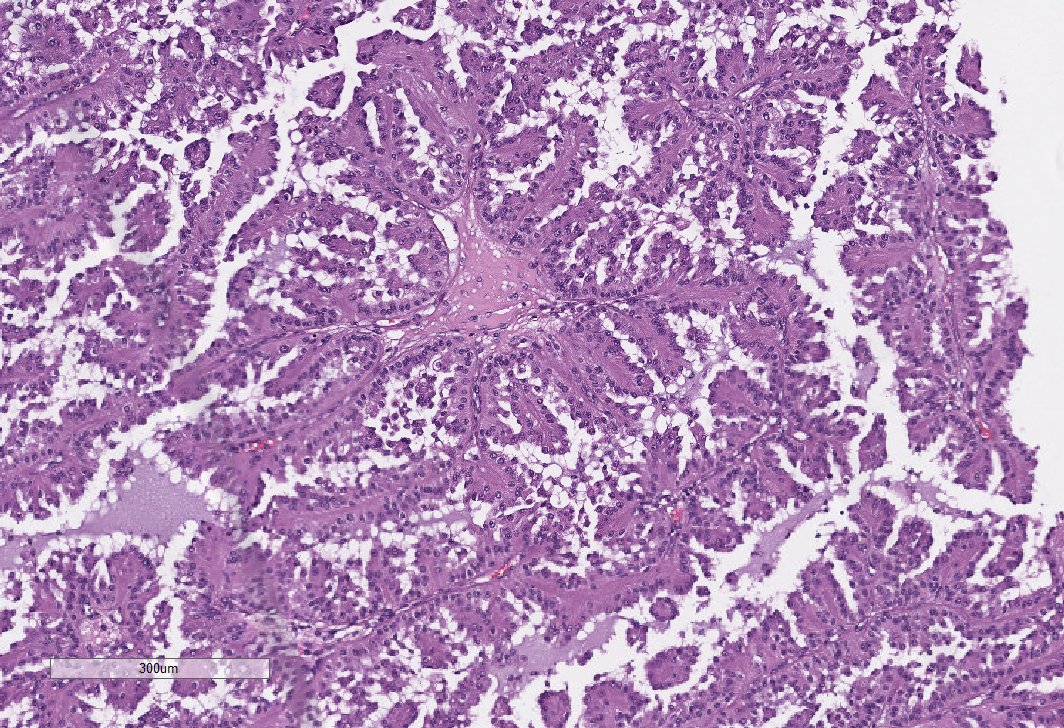
Rib mass in a young male with a renal mass (not biopsied). Morphology was entirely tubulocystic. Thread continued below. 👇 #GUpath 


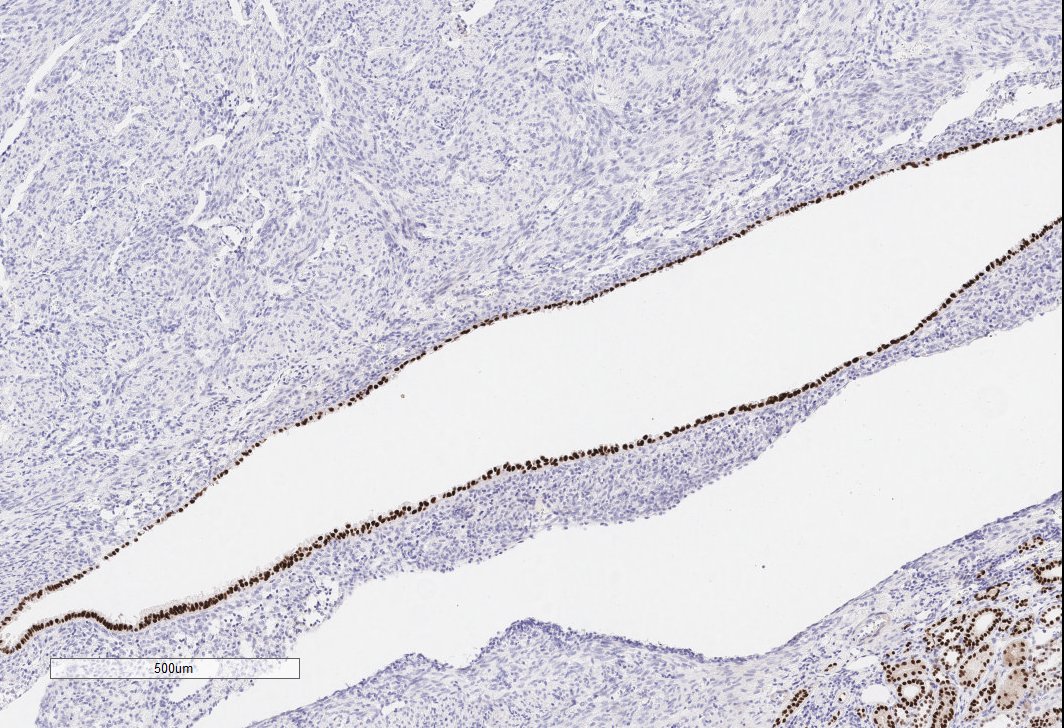
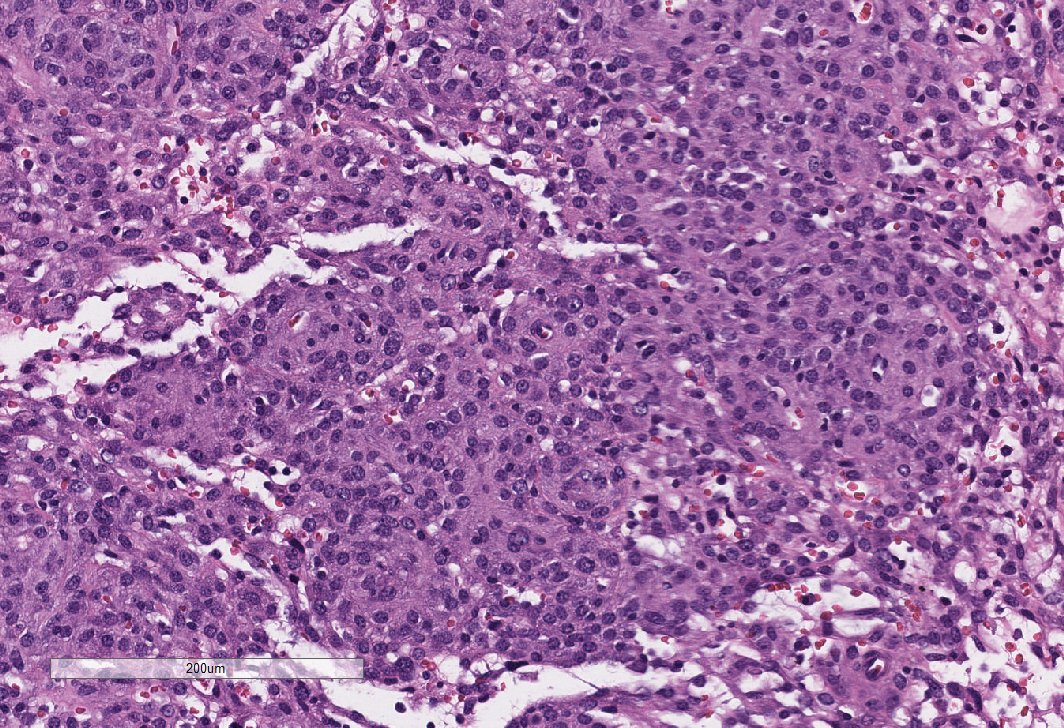
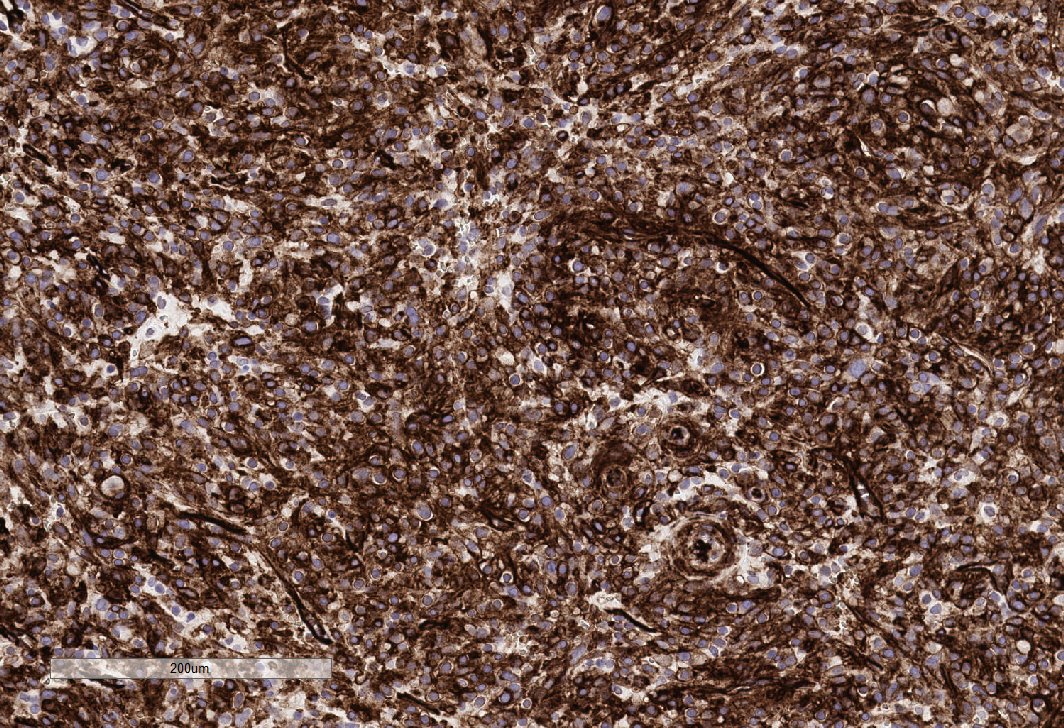
This is what the follow up resection looked like. I received this a few years ago, before we had the FH stain in house. Given the extensive tubulocystic morphology and high grade nuclei, I asked the clinician to test the pt for an FH gene mutation (he was + for the mutation). 👇


Final diagnosis: HLRCC.
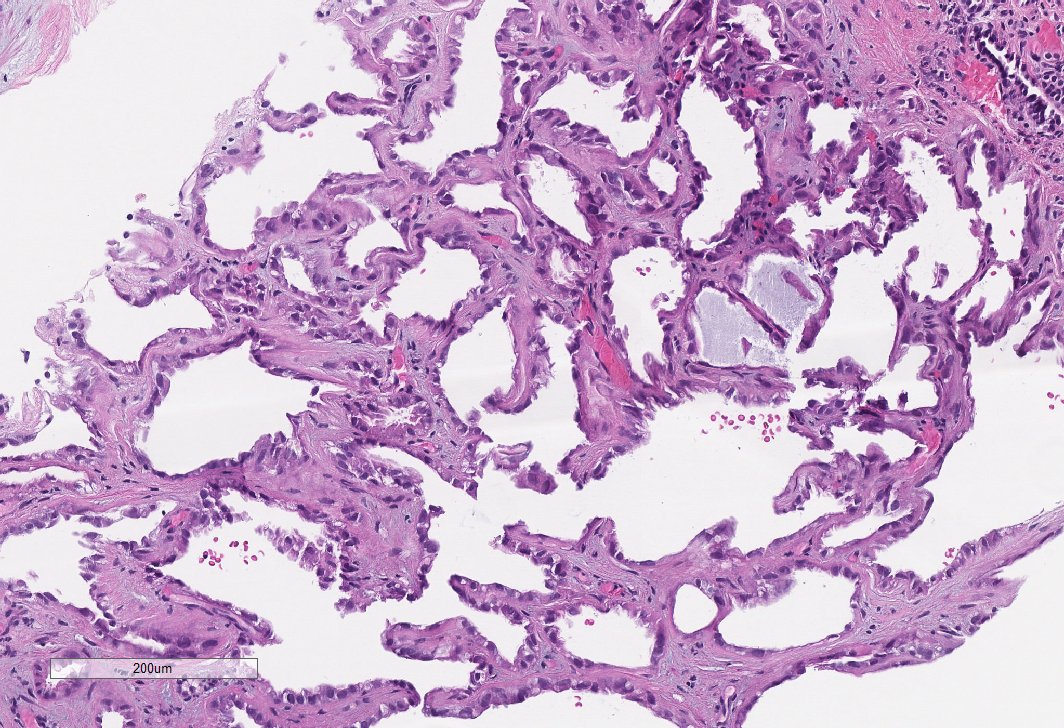
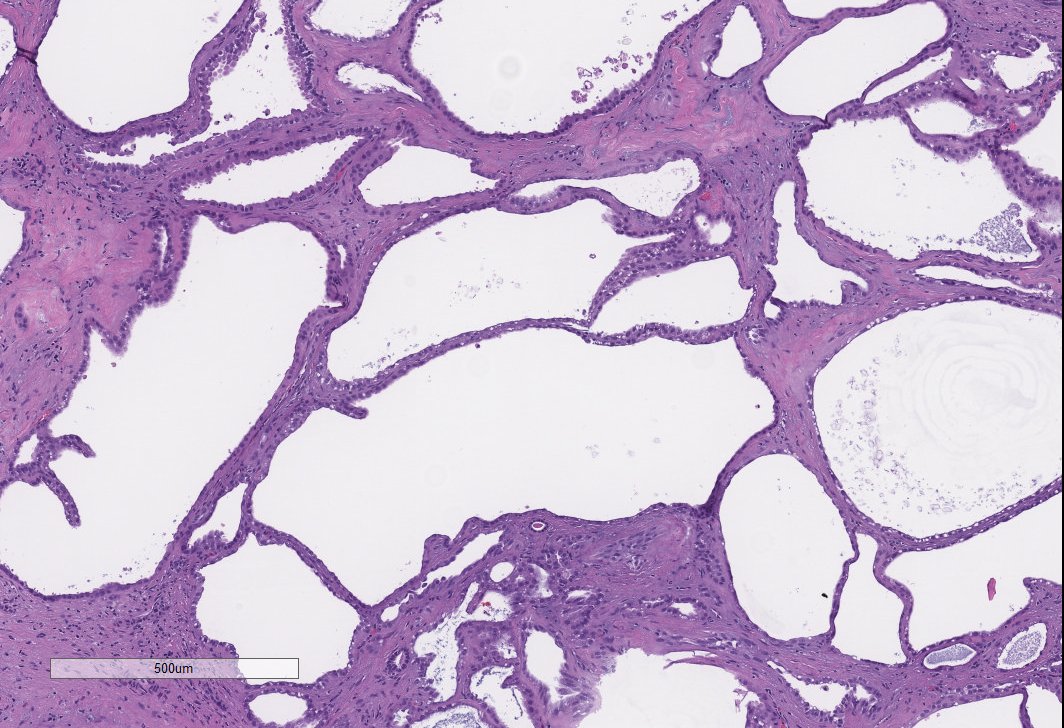
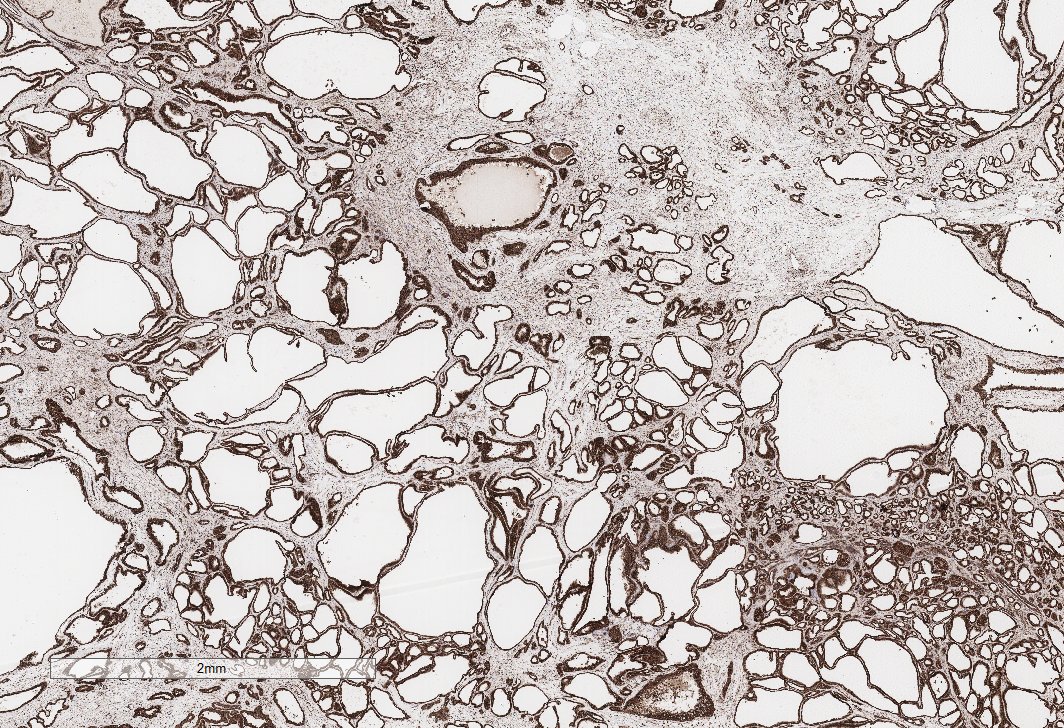
Tumors may be extensively tubulocystic (TC), especially on bx. These are far more common (in my practice) than true TC RCC's. I run the FH stain on all RCCs with TC features.
Bx was signed out as RCC with TC features, clinically exclude HLRCC. #GUpath
Tumors may be extensively tubulocystic (TC), especially on bx. These are far more common (in my practice) than true TC RCC's. I run the FH stain on all RCCs with TC features.
Bx was signed out as RCC with TC features, clinically exclude HLRCC. #GUpath
• • •
Missing some Tweet in this thread? You can try to
force a refresh