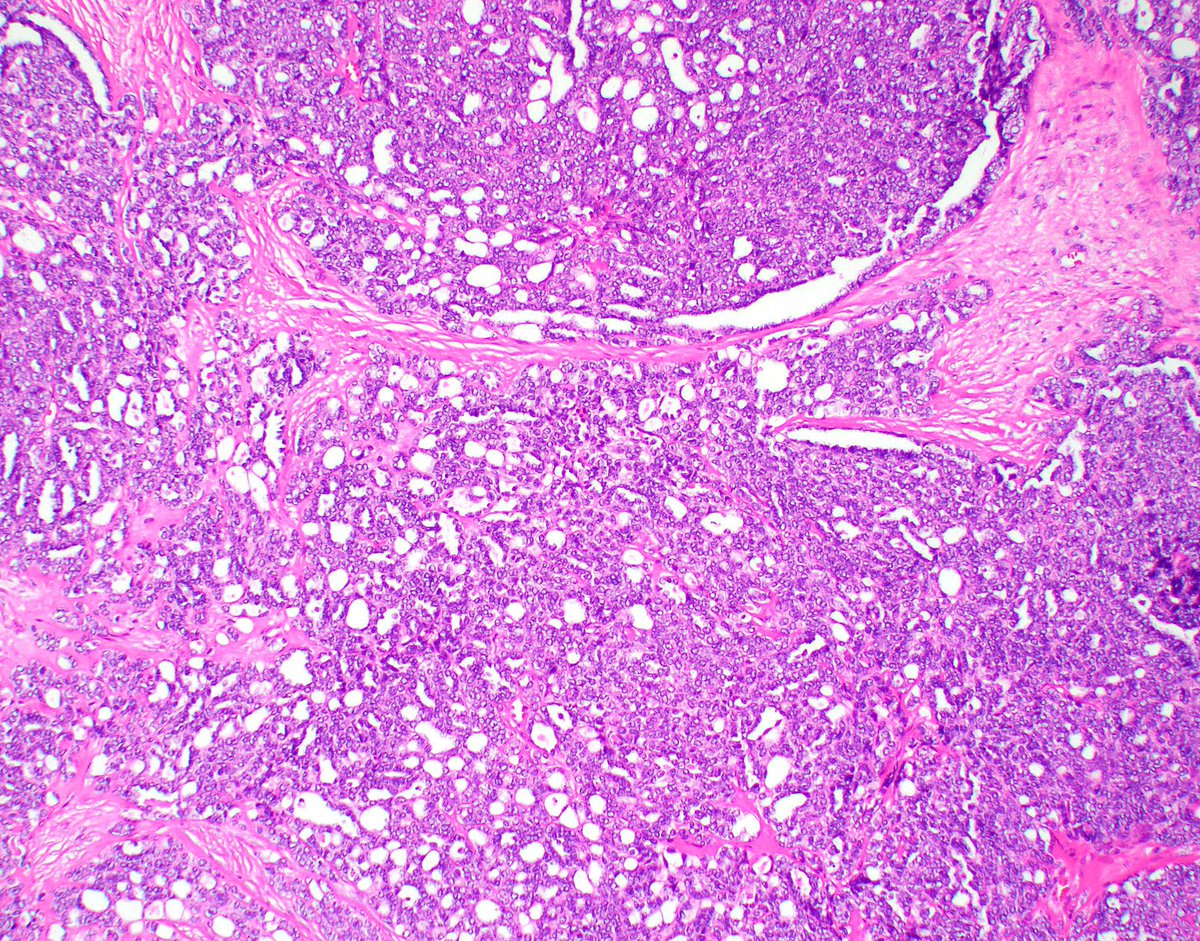
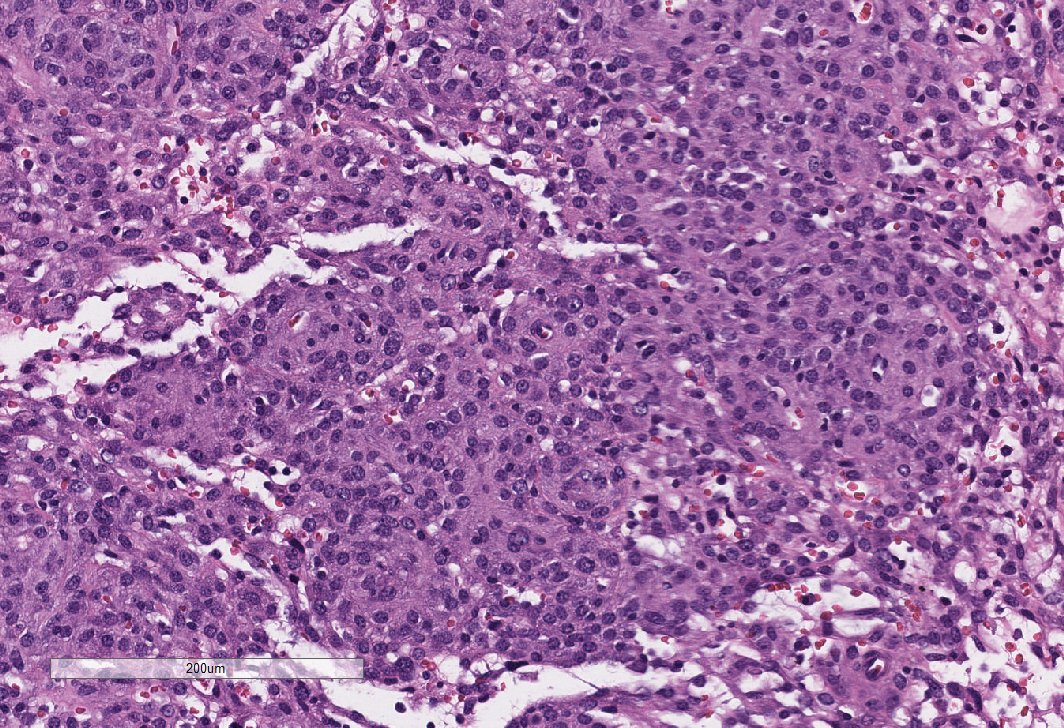
Renal bx from a woman in her late 50s, with a renal mass and metastasis. This biopsy is from the kidney. This was a highly infiltrative, high grade tumor with a desmoplastic background. Continued 👇 #GUpath 


The referring institute reported + PAX8, CK7, - GATA3, CK20, TTF1. O/S diagnosis was collecting duct carcinoma.
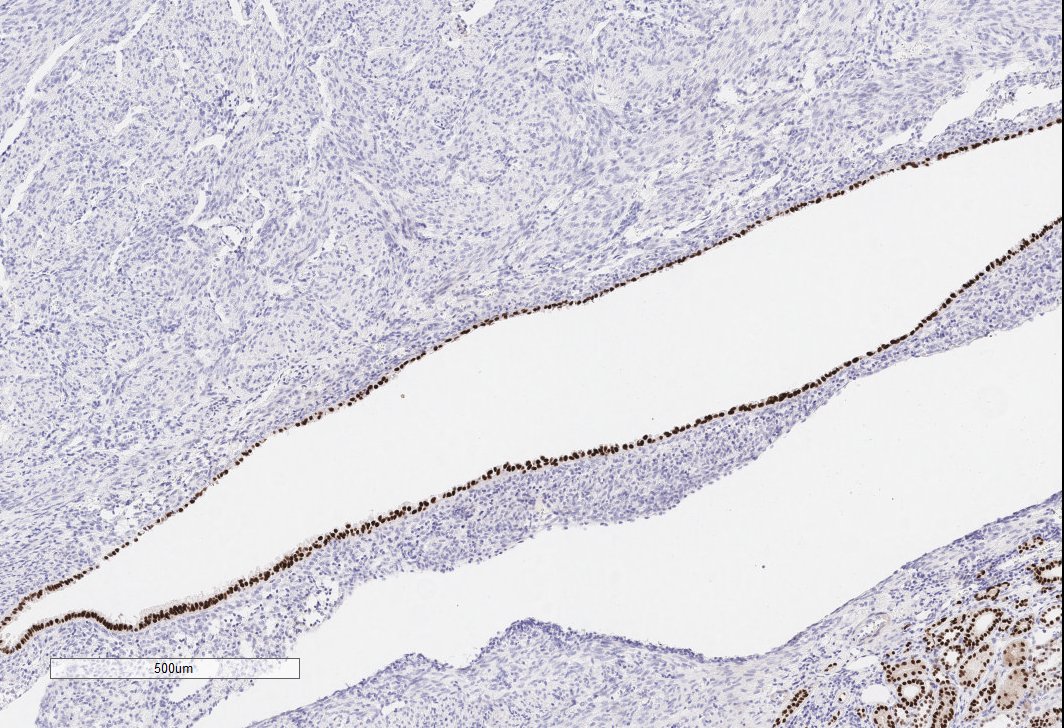
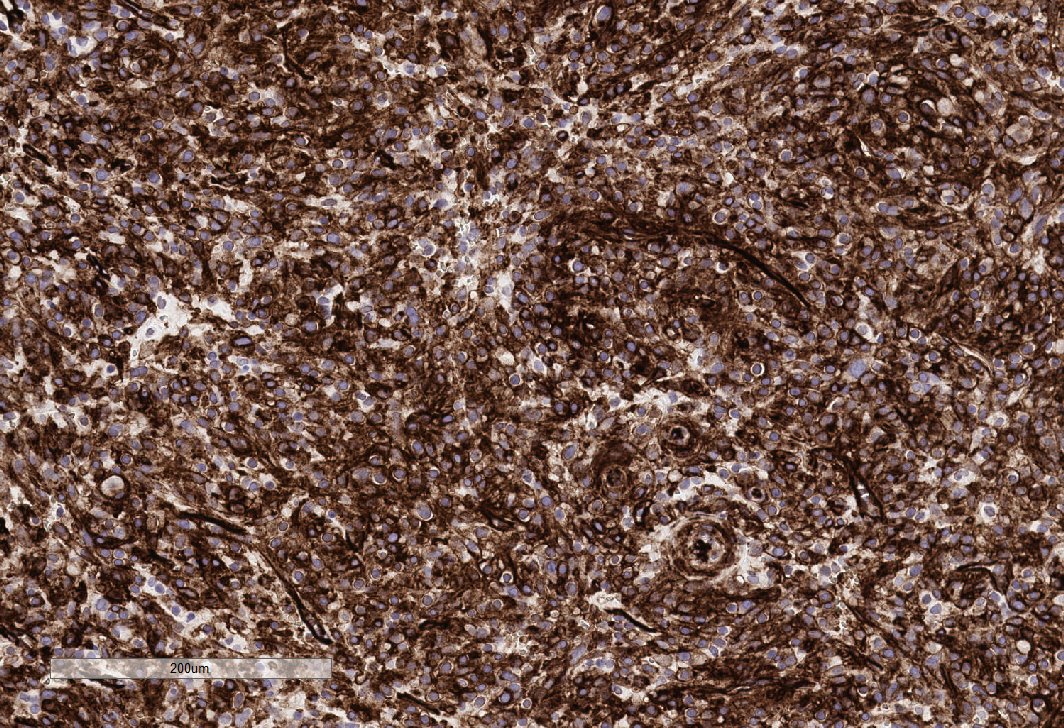
Upon review by us, we realized that the pt was AA and ordered an INI-1 which was negative.
Diagnosis: Renal medullary carcinoma (confirmed by Hb electophoresis) 👇
Upon review by us, we realized that the pt was AA and ordered an INI-1 which was negative.
Diagnosis: Renal medullary carcinoma (confirmed by Hb electophoresis) 👇
True CDC of the kidney is extremely rare and is a diagnosis of exclusion. All tumors that look like a high grade adenoca, automatically get an INI-1. (I always exclude Uca and mets.)
RMC is usually a disease in younger pts, but can present at any age. #GUpath @PavlosMsaouel 👇
RMC is usually a disease in younger pts, but can present at any age. #GUpath @PavlosMsaouel 👇
To underscore the rarity of true collecting duct carcinoma, we see several cases of RMC here at MDA a year (I would guess about 20?) and less than 1 case a year that we call CDC. #GUpath @PavlosMsaouel
• • •
Missing some Tweet in this thread? You can try to
force a refresh