So many great abstracts to peruse for #ASCO20. Some themes: weekly regimens, anti-BCMA therapies, MRD, & high-risk disease. By abstract #, here are 10(ish) #ASCO20 abstracts that stood out to me for their clinical relevance and intrigue. Long thread incoming! #mmsm #ASCO20BD /1
Plenary LBA3: KRd vs. VRd. No data yet until May 28, but this will be relevant no matter what the outcome is! Note that most high-risk patients were not included in this study. Don't think we'll have a final answer on this debate though! meetinglibrary.asco.org/record/186906/… #mmsm #ASCO20BD /2
#100: Phase I trial of Teclistamab, a bispecific BCMA x CD3 T-cell engager, showed reasonable rates of CRS (56%, all <grade 3). ORR was 38% at doses >38.4 ug/kg. 7/9 (78%) responded at highest dose (2 were CR + MRD-neg at 10^-6). #mmsm #ASCO20BD meetinglibrary.asco.org/record/186864/… /3
#8501: Weekly Selinexor/Vd has superior PFS to Vd (~14 vs 9.5 months, HR 0.7) in R/R MM. #8530 shows weekly SKd w/ORR 72%. These weekly S regimens are a bit more tolerable than prior twice weekly S combos. #mmsm #ASCO20BD meetinglibrary.asco.org/record/186143/…
meetinglibrary.asco.org/record/186179/… /4
meetinglibrary.asco.org/record/186179/… /4
#8506: Chaos from the STaMINA trial! Findings from EMN02 and STaMINA have now flip-flopped! EMN02 shows no diff & STaMINA shows PFS benefit for tandem ASCT in high-risk. BUT this was in the as-treated analysis, not intention to treat. #mmsm #ASCO20BD meetinglibrary.asco.org/record/186147/… /5
#8507: VRd +/- Elotuzumab for high-risk myeloma. 103 pts. 7% had PCL. No diff. in median PFS (31 months for Elo/VRd vs. 34 months VRd) or OS (HR 1.28). Is this a reflection of Elo or a prediction for all quadruplets in high-risk disease? #mmsm #ASCO20BD meetinglibrary.asco.org/record/186157/… /6
#8512: Mass Spec in blood vs Next gen flow in marrow on GEM-CESAR trial. Mass Spec identified disease in ~95% of patients who were positive by NGF-MRD. Mass Spec and NGF are complementary for disease detection! #mmsm #ASCO20BD meetinglibrary.asco.org/record/186156/… /7
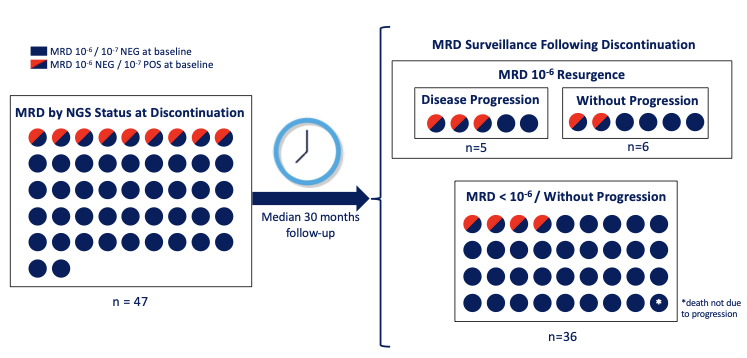
#8514: 73% of MM pts relapsed after converting from MRD-neg to pos. Loss of MRD-neg preceded relapse by 1 yr. Attaining MRD-neg w/in 6 mos. of diagnosis led to HIGHER relapse rate! What does this mean for MRD as an endpoint 4 induction? #mmsm #ASCO20BD meetinglibrary.asco.org/record/186150/… /8
#8526: Cross-study comparison of CANDOR & MMY1001. Once weekly carfilzomib 70 mg/m2 is similar in efficacy and toxicity to twice weekly carfilzomib 56 mg/m2. Good news in the age of COVID where once weekly infusions has many advantages. #mmsm #ASCO20BD meetinglibrary.asco.org/record/186186/… /9
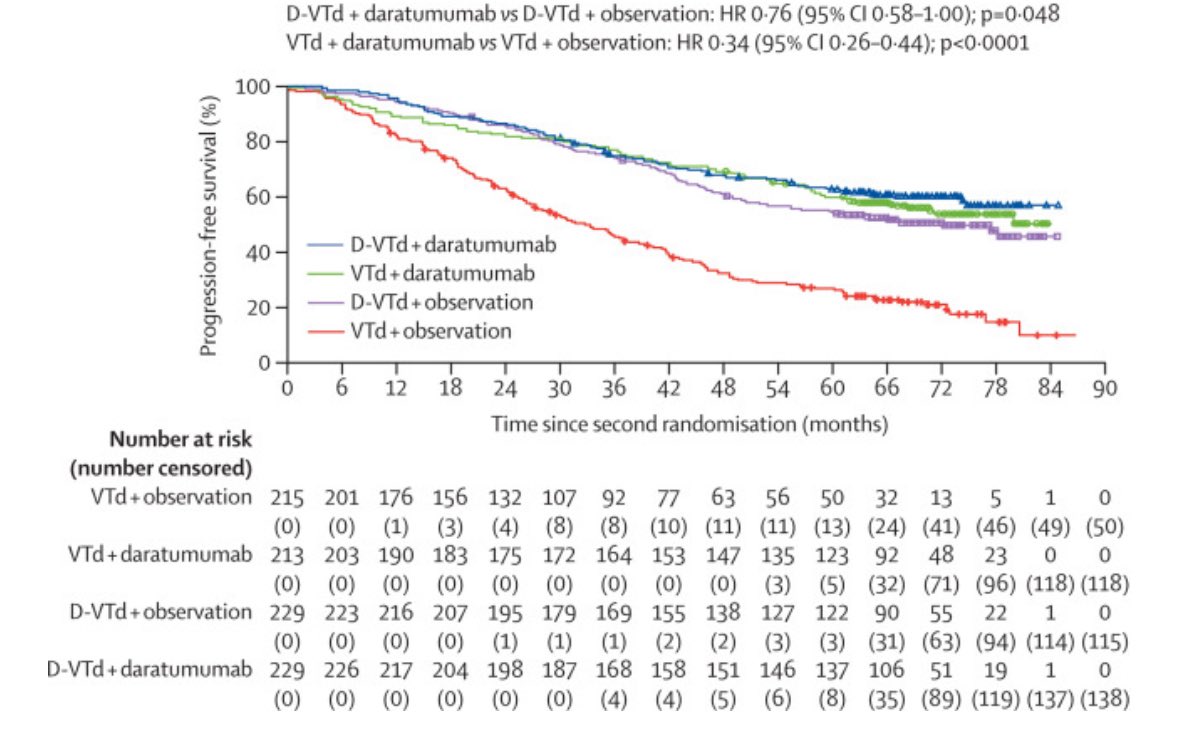
#8540: Meta-analysis of randomized phase 3 trials evaluating efficacy of Dara in high-risk MM. Shows that Dara led to improved PFS with little heterogeneity. We need a randomized study using dara in high-risk patients! #mmsm #ASCO20BD meetinglibrary.asco.org/record/187638/… /10
#8543: Obesity in multiple myeloma was PROTECTIVE in an analysis of nearly 6K patients on clinical trials. OS HR 0.84 (95% CI 0.75-0.95). This brings up some interesting theories as to why – reserve against sarcopenia/cachexia? #mmsm #ASCO20BD meetinglibrary.asco.org/record/186173/… /11
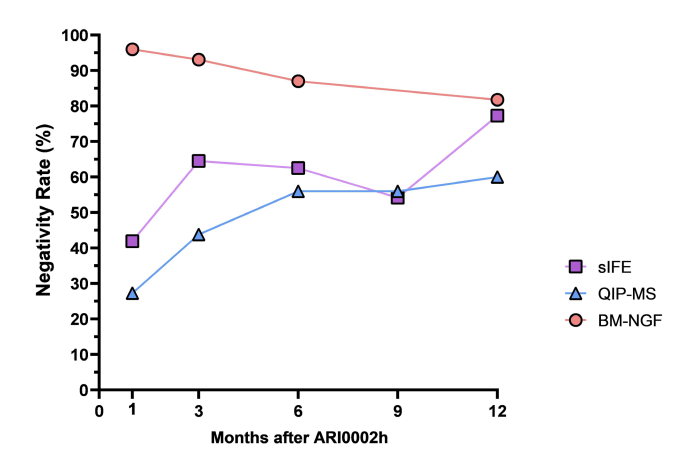
BONUS: #8513 (disclosure-I am author on study). Mass spec in blood vs NGS in marrow for MRD eval in MM. LC-MS in blood may reach or exceed sensitivity of NGS (10^-5 - 10^-6), and is an excellent prognosticator. More on this next week! meetinglibrary.asco.org/record/186146/… #mmsm #ASCO20BD /12
• • •
Missing some Tweet in this thread? You can try to
force a refresh