Asst Professor at UChicago, interim director myeloma program. I tweet about: Myeloma & MRD. https://t.co/mPeWg1QjCo



 Briefly, before I go into our findings. The concept for this study originated 7 years ago with our patients. I was a fellow, and the most common question from our deep responding patients was, "What happens if I stop treatment?" We didn't know, of course, so we tried to answer it
Briefly, before I go into our findings. The concept for this study originated 7 years ago with our patients. I was a fellow, and the most common question from our deep responding patients was, "What happens if I stop treatment?" We didn't know, of course, so we tried to answer it

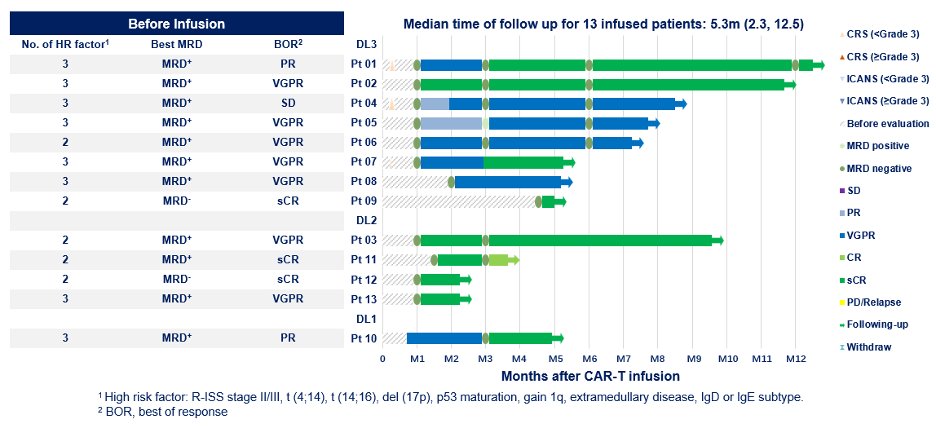
 2) Most patients are peripheral blood MS (+) early post-CAR T because of M-protein kinetics + immunoglobulin recycling
2) Most patients are peripheral blood MS (+) early post-CAR T because of M-protein kinetics + immunoglobulin recycling 
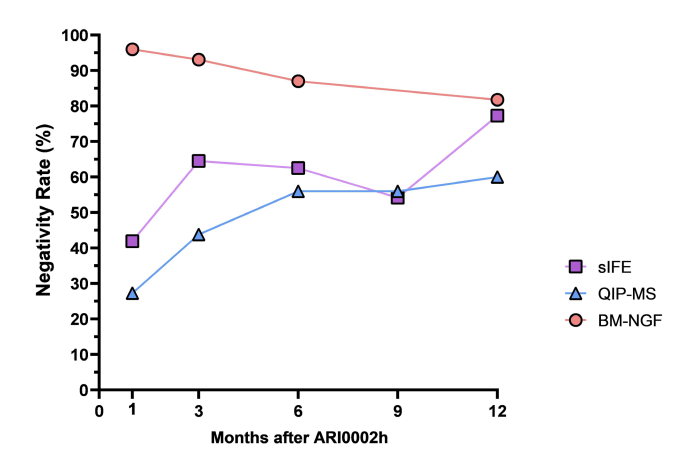
 There’s also great MRD data.
There’s also great MRD data.






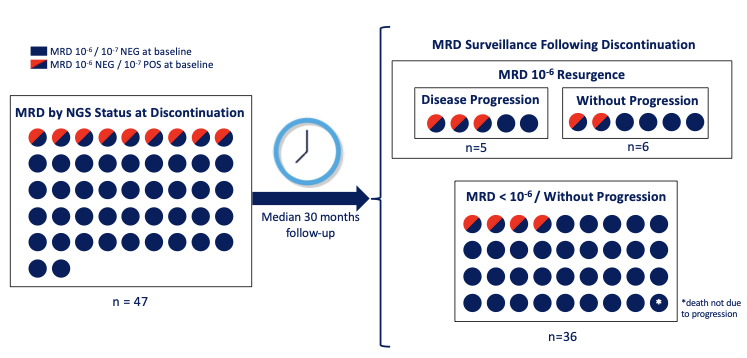
 We had paired IMWG response status and bone marrow MRD by NGS status for many of the patients still in response at the end of 4 cycles.
We had paired IMWG response status and bone marrow MRD by NGS status for many of the patients still in response at the end of 4 cycles. 

 Patients could have stem cells collected on study but this was a transplant-deferred approach. 88% had SCT collected - median 8.26 x 10^6 CD34+/kg!
Patients could have stem cells collected on study but this was a transplant-deferred approach. 88% had SCT collected - median 8.26 x 10^6 CD34+/kg! 
 Some other key demographic:
Some other key demographic: