
1/ With R~1 in many places despite social distancing & (possibly)⬆️testing, we need to precisely understand why, where &, if possible, how transmission is still happening so we can refine our response to get it down further
This is what we did against Ebola in West Africa
This is what we did against Ebola in West Africa
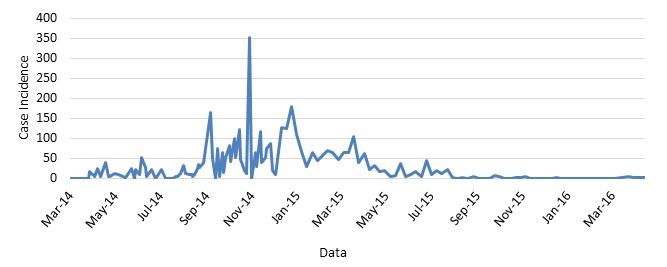
2/ Once main broad strategies - #TestTraceIsolate, behavior change – were put into play, transmission came down but still lingered
We serially found gaps, tightened/tailored response, got transmission down & then repeated this process over and over again to drill down to zero
We serially found gaps, tightened/tailored response, got transmission down & then repeated this process over and over again to drill down to zero
3/ Based on ‘verbal autopsies’ used in health systems strengthening to discern medical causes of each death & more importantly systems gaps that failed to prevent it, we should do ‘epidemiological autopsies’ to understand the story – the why & how – behind every new infection
4/ We can then use that information to strengthen identified gaps & tailor strategies if cases are mainly from certain scenarios or clustered in certain areas or among particular groups (eg, nursing homes)
5/ With Ebola, we learned in one hotspot cases were due to unsafe burials. When we probed further, it wasn't cause communities weren’t bought into safe burials but that we were slow to collect deceased bodies. We increased cars, fuels & drivers for this purpose & closed this gap
6/ In another place, cases were still happening cause communities didn’t trust us & hid their sick & secretly buried those who died at night. We deployed anthropologists to intensively engage w/these communities who eventually started working with us to stop the virus’s spread
7/ We can apply a similar approach for COVID
With R~1, what proportion of current cases are happening in high-risk settings, among essential workers, or particular neighborhoods or groups? Or are cases from the general population due to breaches in social distancing?
With R~1, what proportion of current cases are happening in high-risk settings, among essential workers, or particular neighborhoods or groups? Or are cases from the general population due to breaches in social distancing?
8/ Based on the answer, we know where to redouble our efforts. If mainly high-risk settings, what do we need to do better? If among essential workers, is it among particular subsets eg, grocery store clerks? If so, what protocols or PPE do we need to better protect them?
9/ These drivers likely vary by place & even neighborhood & this analysis needs to be done site-specifically.
In this paper, my former co-resident @yhgrad shows how transmission in NYC correlated with commuting patterns.
Factors are often hyperlocal
In this paper, my former co-resident @yhgrad shows how transmission in NYC correlated with commuting patterns.
Factors are often hyperlocal
10/ We should supplement⬆️broad strategies - #TestTraceIsolate & protections (eg, masks) - with nuanced analysis of new cases (if not already being done this way) to keep focus on how/why transmission is happening & as my colleague @JeanMombouli says "tighten the screws"

