1/ Covid (@UCSF) Chronicles, Day 65
It’s Thursday, Grand Rounds day: bit.ly/3bTcpP9. 5 topics: state of the pandemic (w/ focus on Covid in children); the new Kawasaki-like syndrome in kids; updates in therapies/vaccines; & abnormal clotting in Covid. Highlights below…
It’s Thursday, Grand Rounds day: bit.ly/3bTcpP9. 5 topics: state of the pandemic (w/ focus on Covid in children); the new Kawasaki-like syndrome in kids; updates in therapies/vaccines; & abnormal clotting in Covid. Highlights below…
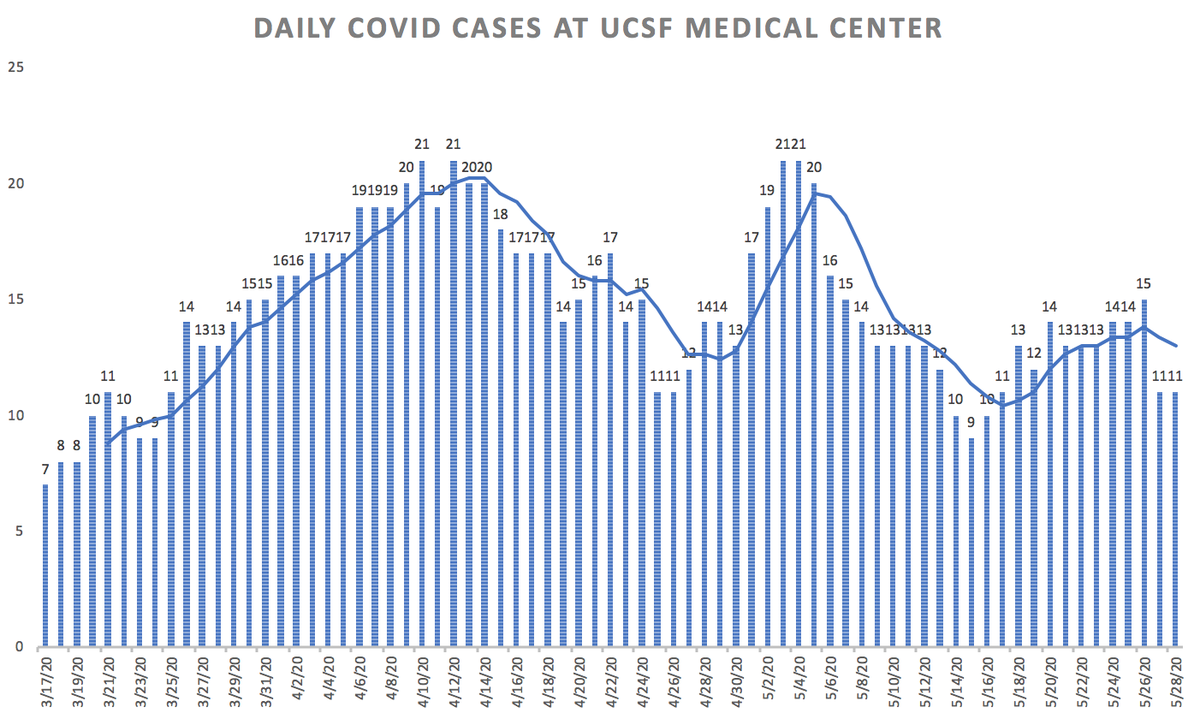
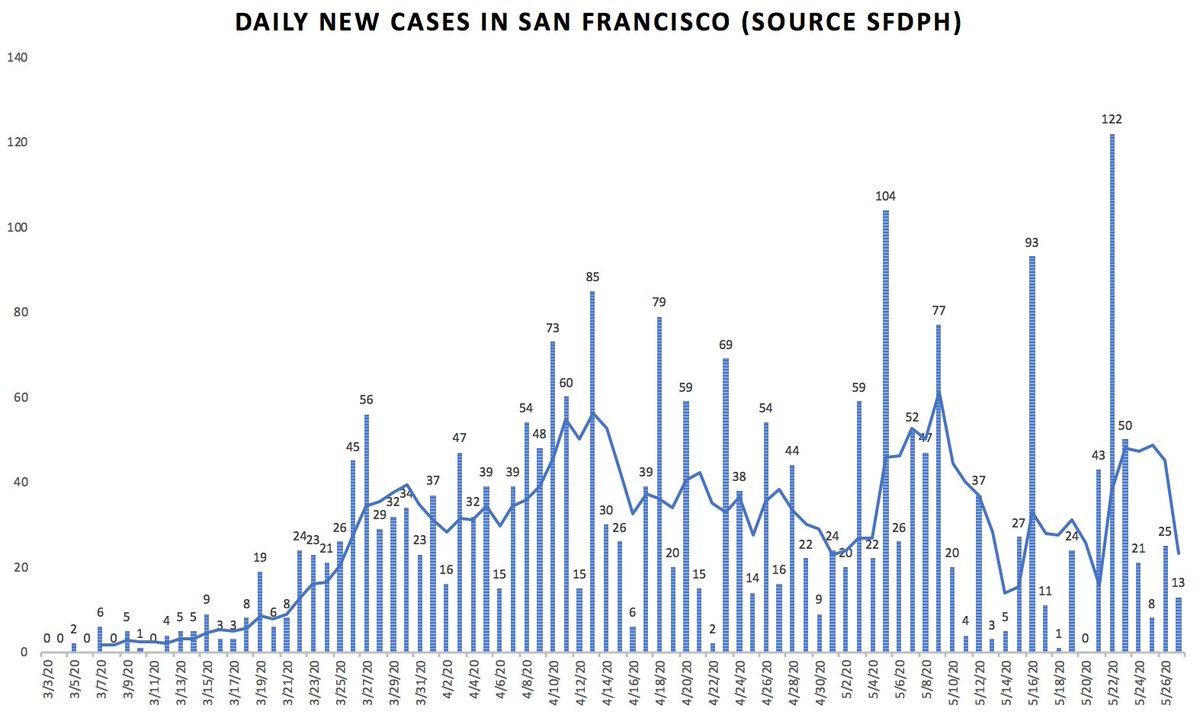
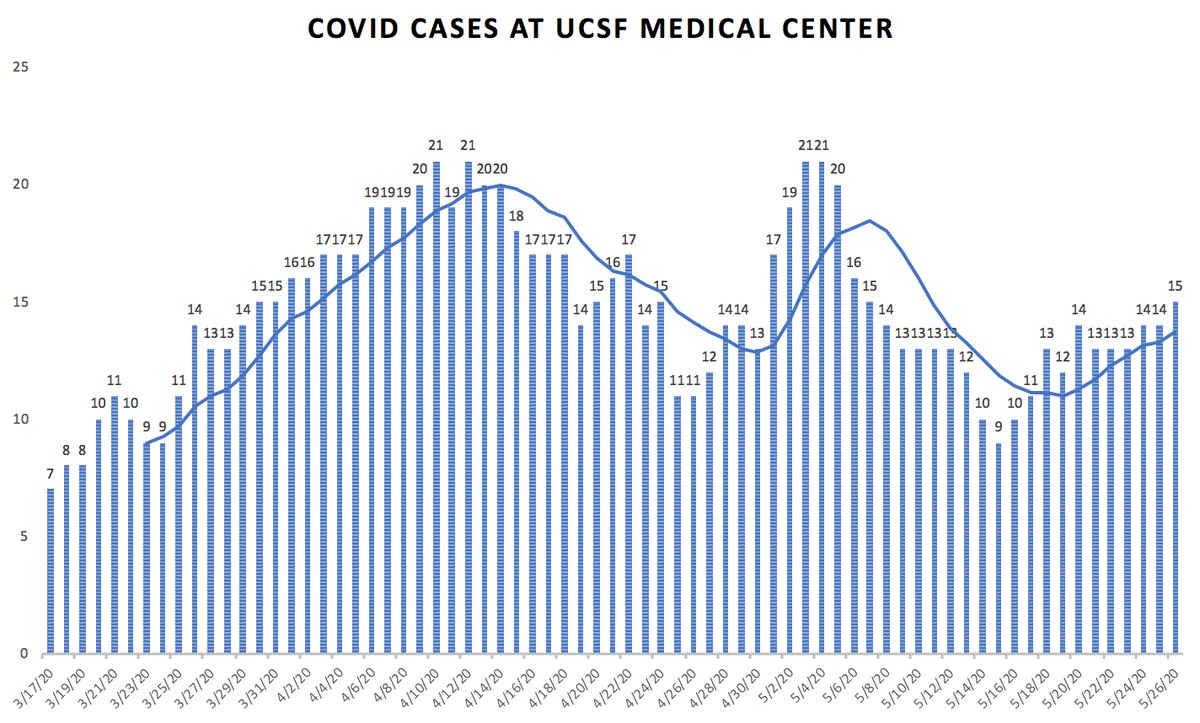
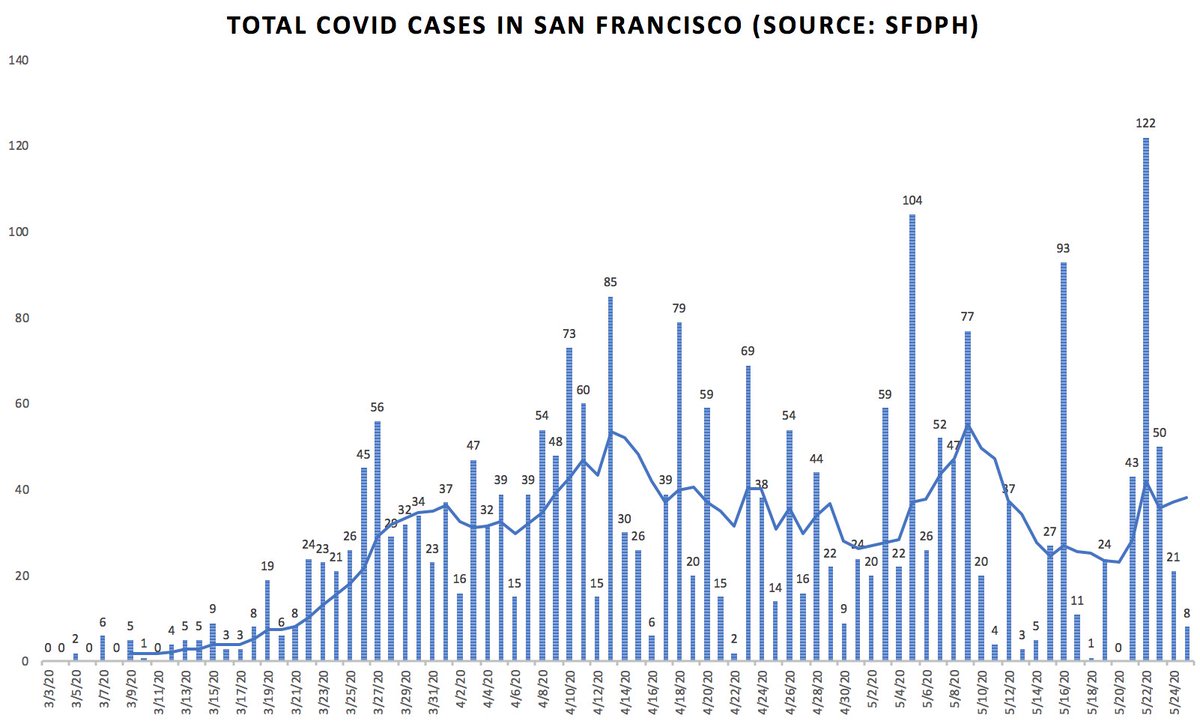
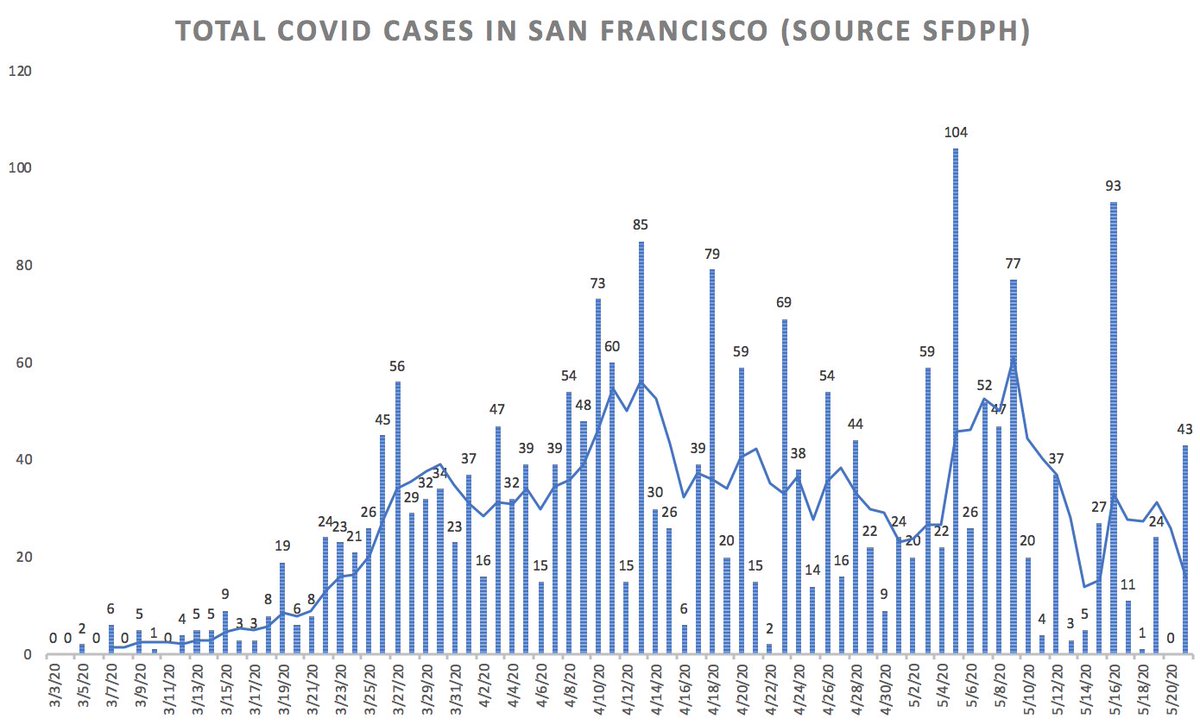
2/ First, San Francisco update. @UCSFHospitals, 13 pts in hospital, 5 on vents (Fig on L), stable. SF Covid data a bit noisy but overall stable: new cases running ~25/d (Fig R), w/ total of 61 patients in SF hospitals (22 in ICUs). Total deaths in SF since start of pandemic: 37. 

3/ To Grand Rounds:
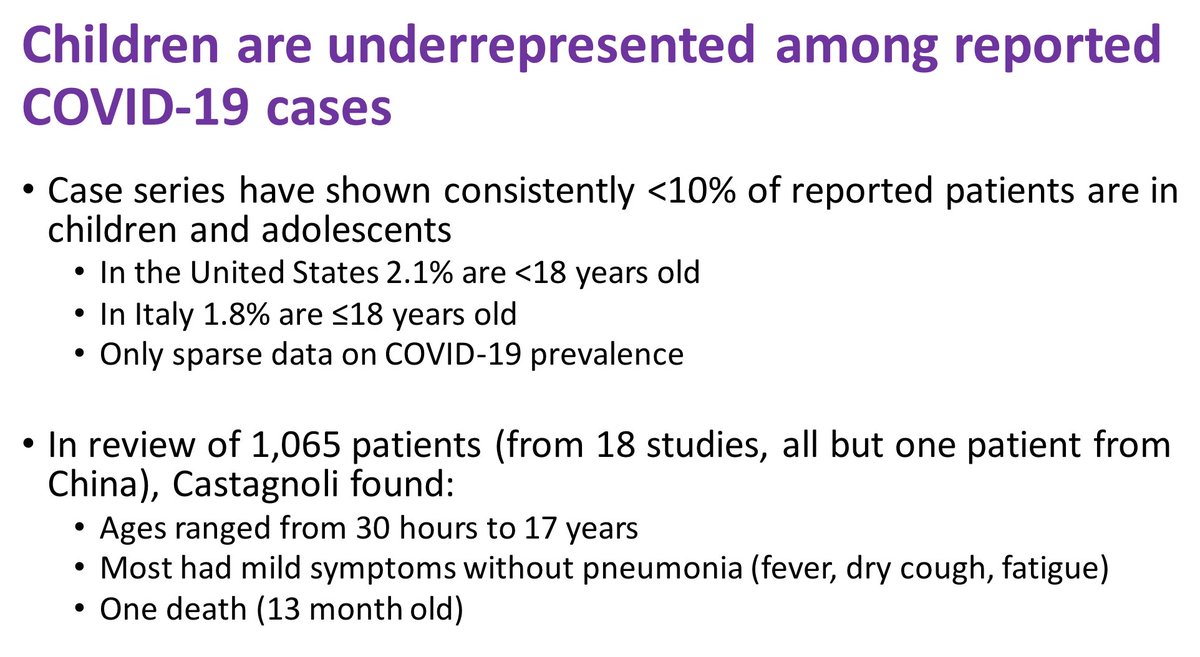
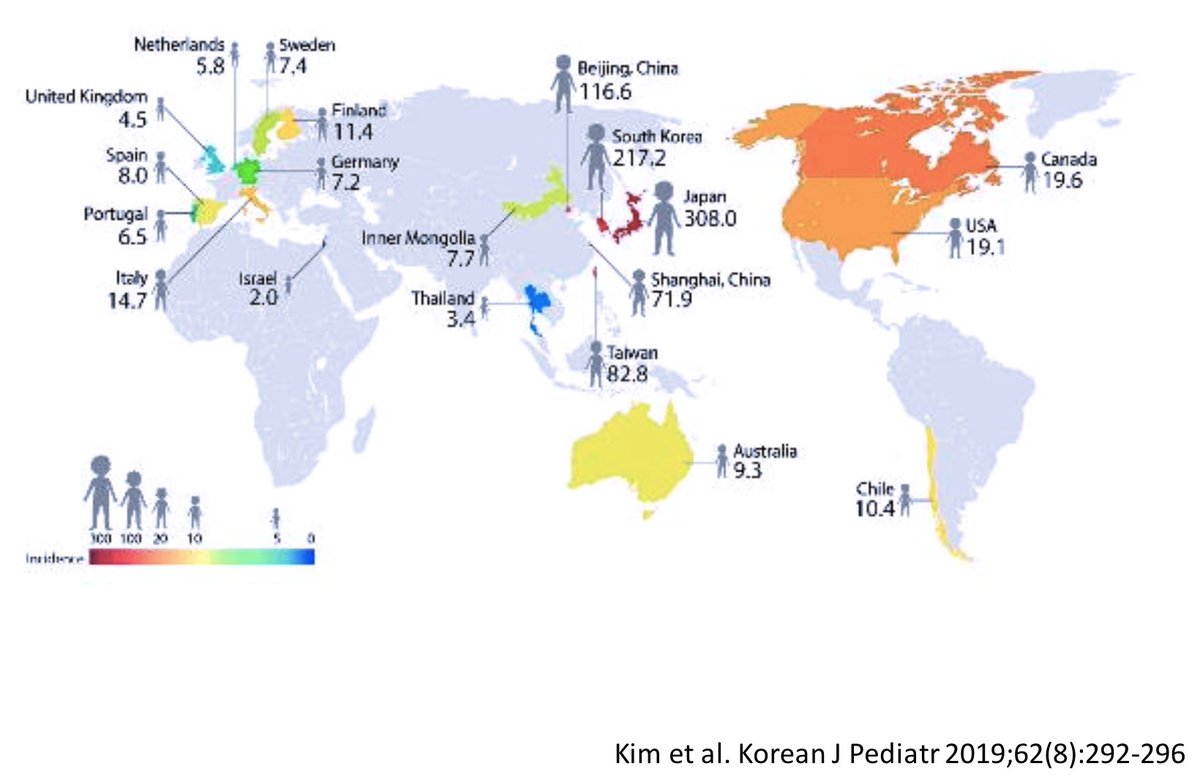
@ 6:20 George Rutherford highlights low incidence of severe disease in children. It’s not just that kids rarely get sick – evidence (@ 10:10) says that kids mostly catch Covid from adults, rarely other way around. “A one-way street, from older to younger.”
@ 6:20 George Rutherford highlights low incidence of severe disease in children. It’s not just that kids rarely get sick – evidence (@ 10:10) says that kids mostly catch Covid from adults, rarely other way around. “A one-way street, from older to younger.”
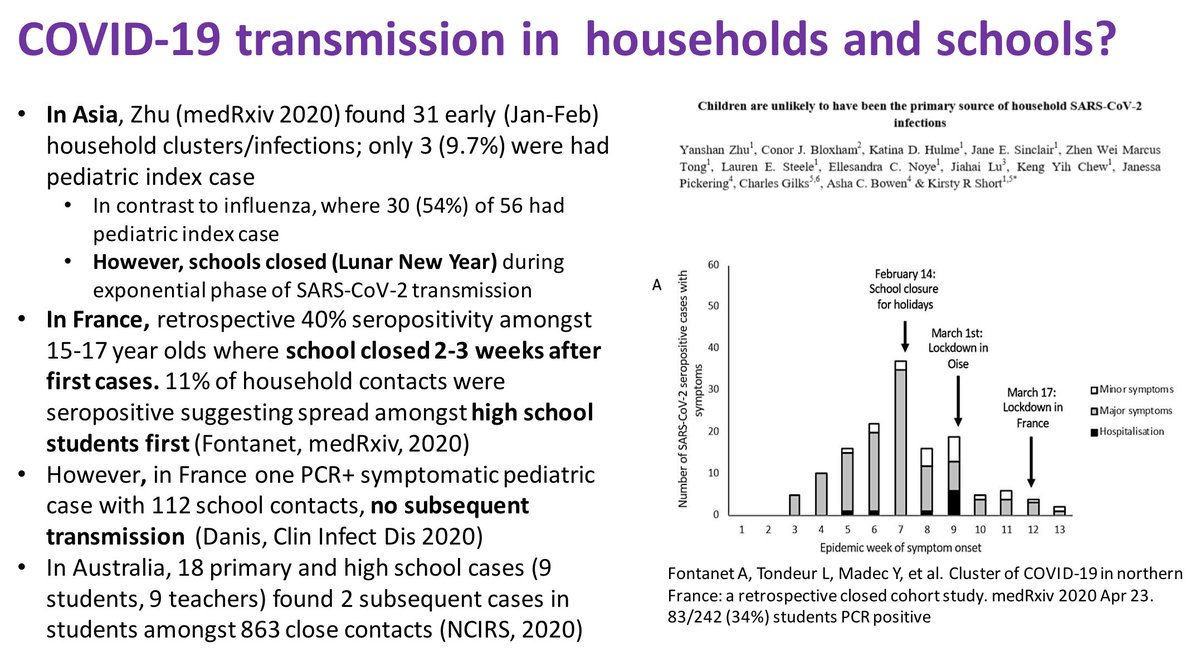
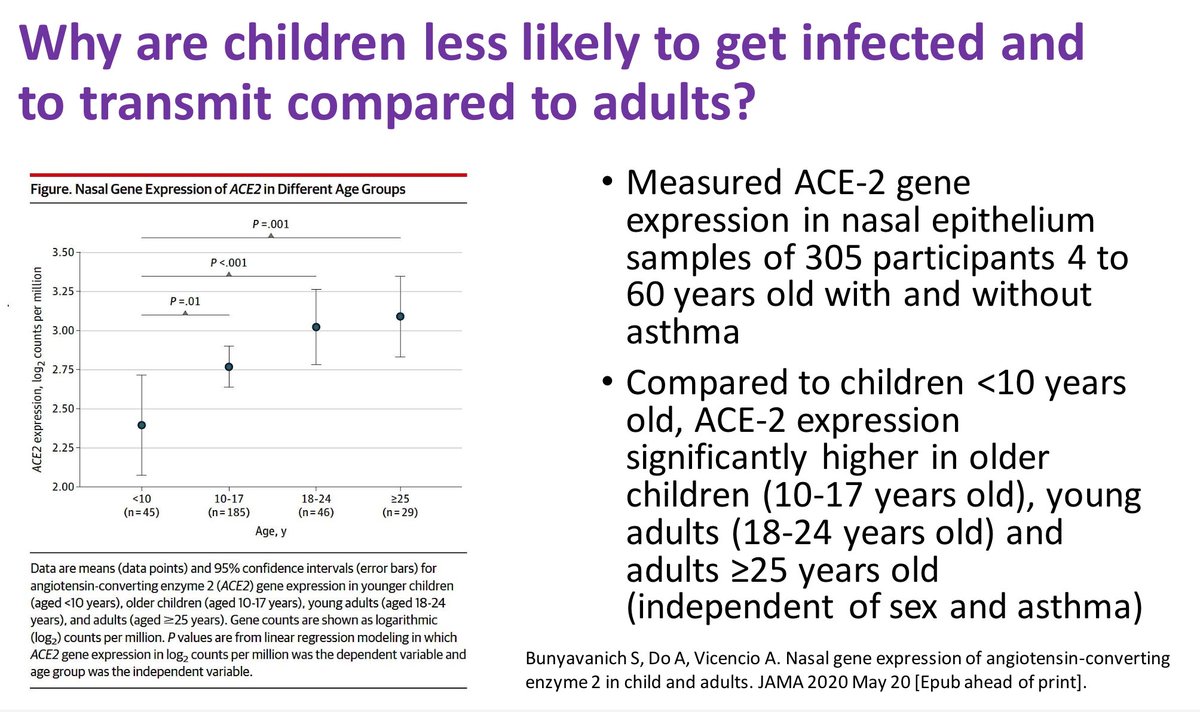
4/ This is gobsmacking – in influenza, kids play a huge role in transmission. Why is Covid so different? @ 14:25: New JAMA study: lower ACE-2 gene expression in nasal epithelium of kids. Might mean that SARS-CoV-2 can’t take root in kids’ noses. If so, a rare lucky break in Covid
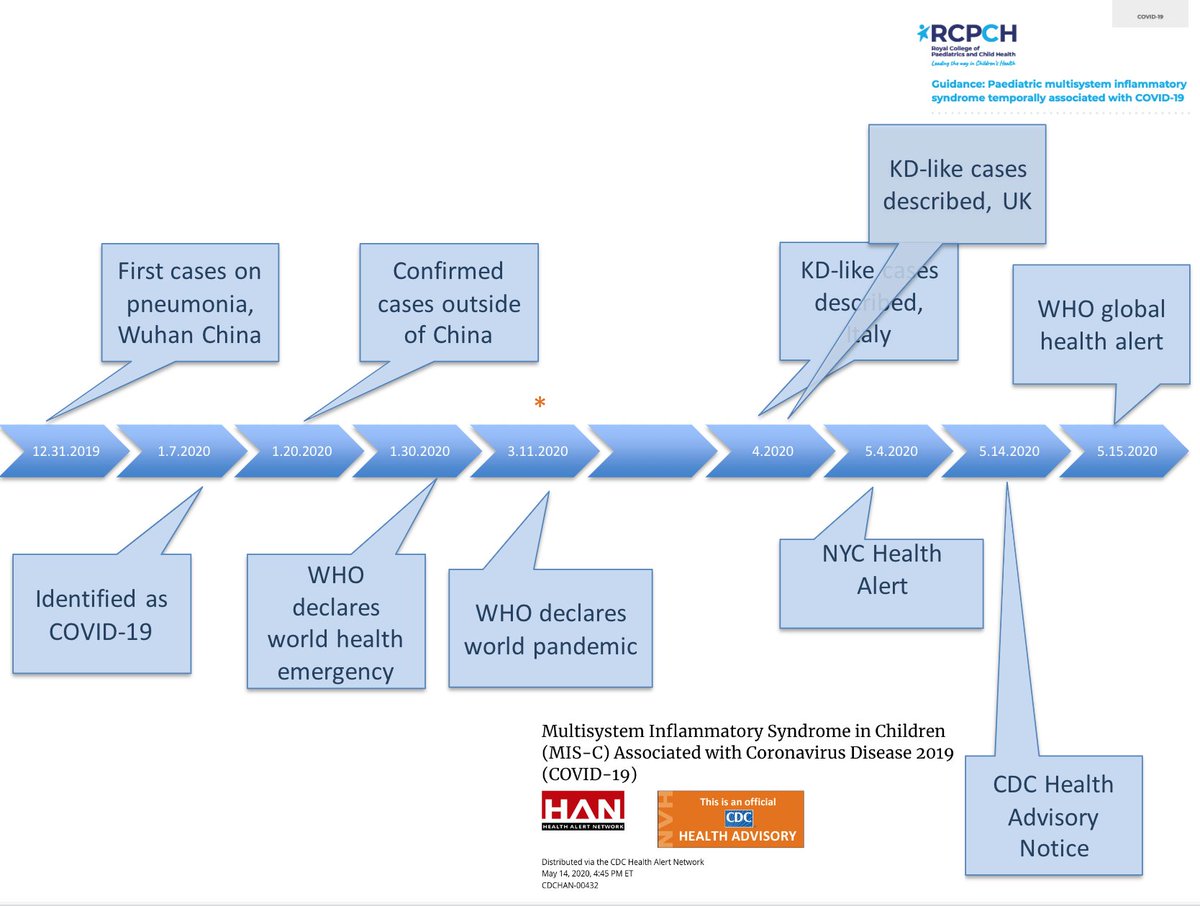
5/ But, alas, kids aren’t off the hook just yet. China experience was that few kids got sick from Covid. Then, 1 month ago, Multisystem Inflammatory Syndrome in Children (MIS-C) described in Italy, UK, then U.S. @ 1:24:00, peds rheumatologist Susan Kim walks us through timeline.
6/ @ 1:28:30, Kim describes Kawasaki syndrome (KS). Without treatment, 25% of KS patients will have damage to coronary arteries; goes down to <5% with treatment (aspirin and immunoglobulins (IvIG)). Not clear yet if MIS-C will respond to similar treatment; it’s being studied.
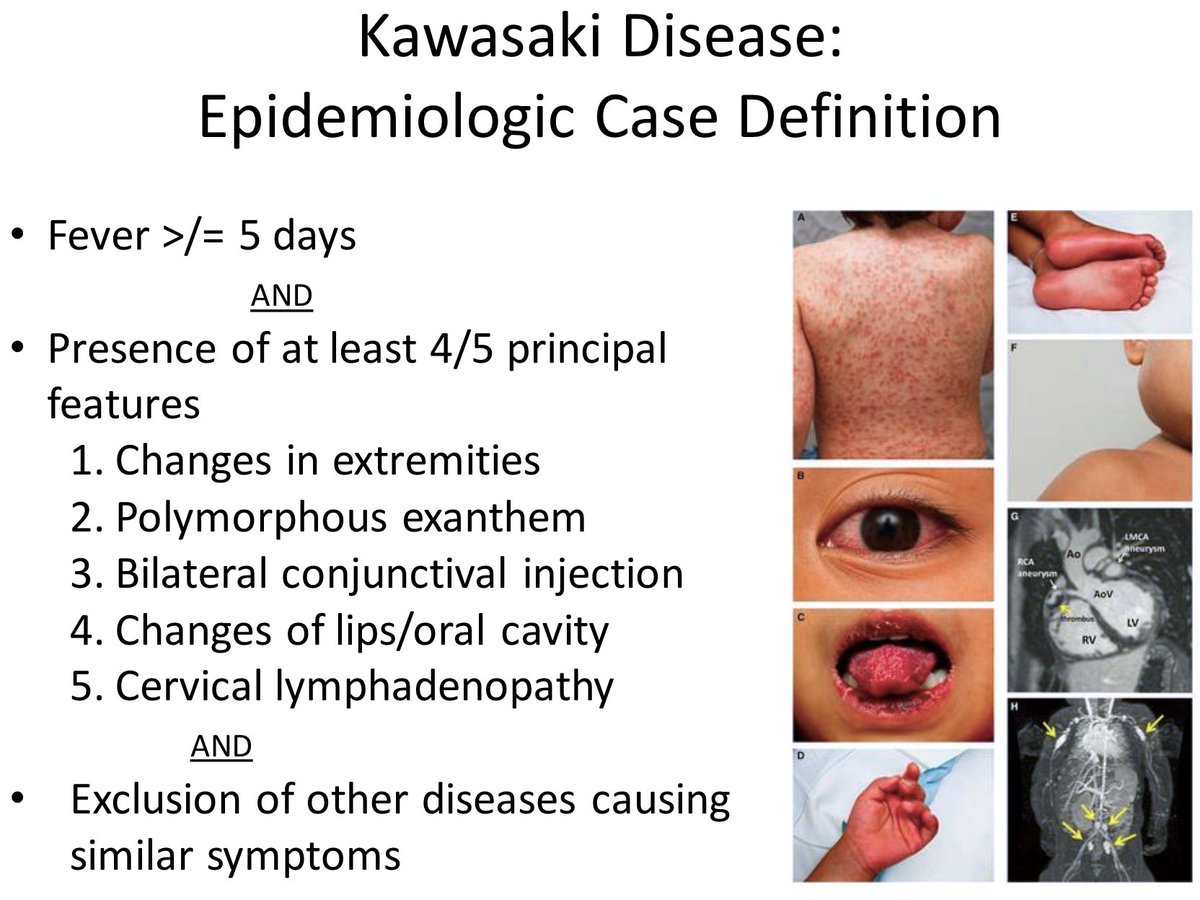
7/ Kawasaki’s is very geographically dependent: not too unusual in Asia, super-rare in U.S. Yet, astoundingly, no MIS-C seen in China/Japan Covid cases (despite carefully seeking it, @ 1:31:37). Do genes that predispose to KS somehow protect kids against MIS-C? Still a mystery.
8/ @ 18:05: George Rutherford favors reopening U.S. schools, carefully. Should be different am/pm kindergarten groups; “The whole point is to keep mixing to a minimum & maintain distancing.” Masks are key. MIS-C doesn’t change his thinking re: reopening schools; it’s too rare.
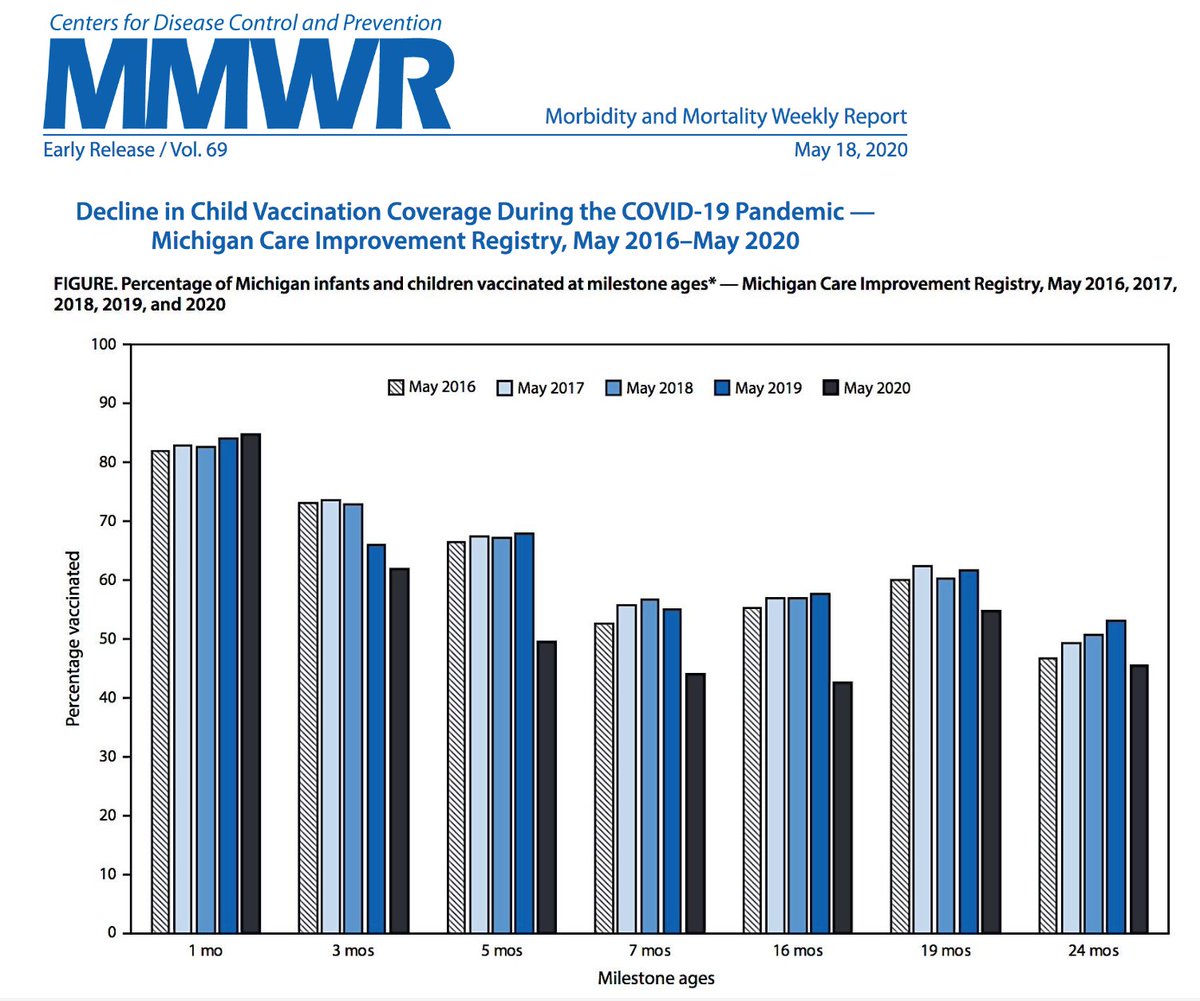
9/ George’s last point re: kids: “In adults, we wonder where the MI’s went; pediatricians wonder where the kids went” when due for vaccines. Big fall in vaccinations; GR predicts we’ll soon see outbreaks of pertussis & measles. Ironic as we struggle desperately for Covid vaccine.
10/ Moving off peds, @ 20:10 I asked Rutherford about the interrelationship between distancing & masks. “I think masks are more important than social distancing… if I had to choose one, I’d choose masks.” “We’re trying to prevent asymptomatic people from transmitting…”
11/ @ 21:30: Early message in Covid was that masks only help others, but GR confirms they also help wearer – just not as much as they prevent transmission to others. It would be great if this message got out more – masks aren’t just an act of charity, they’re also self-interest.
12/ Finally, @ 23:50, I asked how much George worries about fomites. "It’s not as worrisome as somebody sneezing in your face, but you ignore it at your peril.” He’d worry about a metal rail in a public place (like a subway), but doesn’t fret re: touching shopping bags or mail.
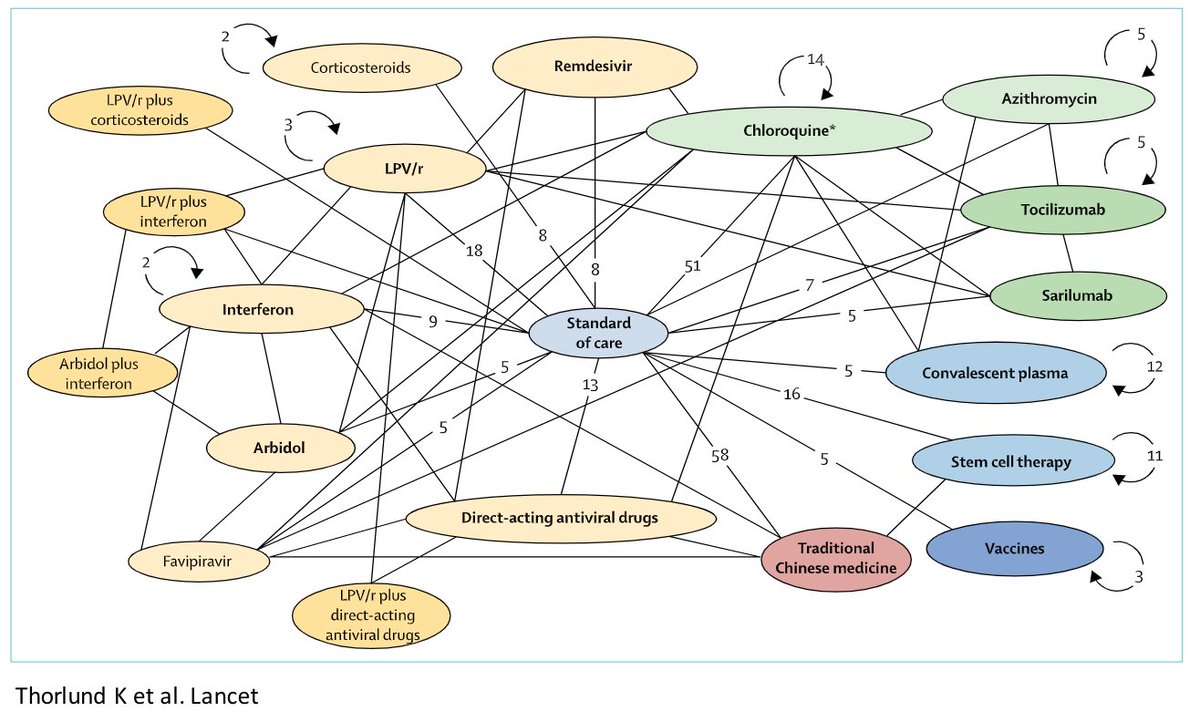
13/ @ 24:50, @annieluet (Luetkemeyer) on treatments. Many candidates, 2 types of targets: antiviral vs. drugs that modify immune system. She makes point that combo Rx might be key. Theoretically, one from each category, but in HIV, turned out that multiple antivirals worked best.
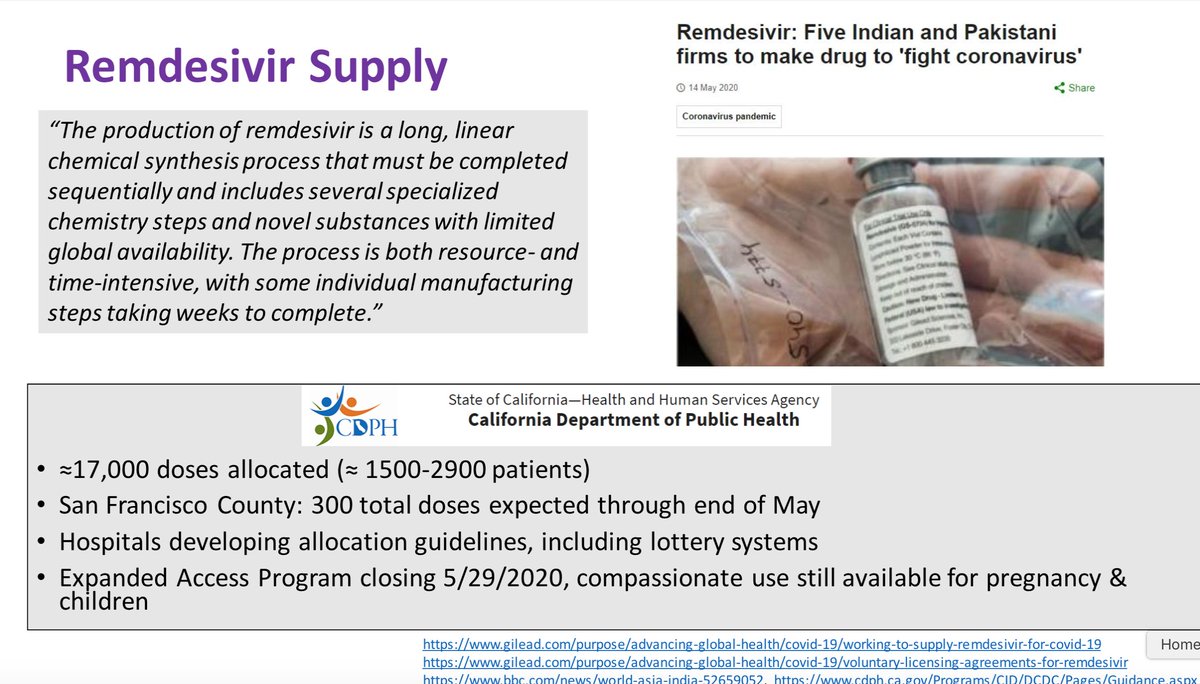
14/ @ 29:02: Remdesivir “isn’t easy to make.” @GileadSciences giving license to generic makers outside U.S. to ramp up production. There’s a nat'l shortage of Remdesivir (incl. in SF) – hospitals are developing triage rules, some using lotteries to decide who gets it. Troubling.
15/ We’re still waiting for better studies of Remdesivir, incl. to tell us if it’s useful in patients w/ milder disease, & if using it in combo w/ other drugs is helpful. Unfortunately, it’s IV only, which thwarts possibility of giving it earlier in course of illness (@ 41:06).
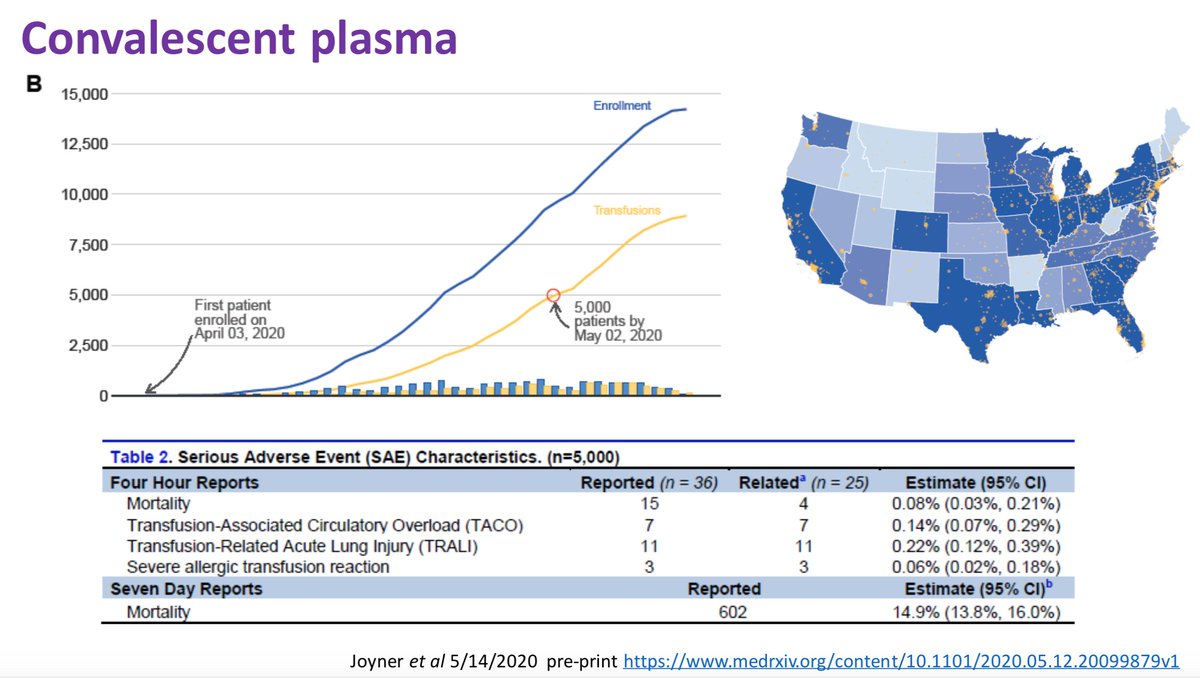
16/ @ 34:10, on use of interferon beta: hint of benefit when started early, yet no mortality benefit seen (but limited: trial had no deaths in treatment & control groups). @ 36:25, re: convalescent plasma: seems safe but still no evidence for mortality benefit. Studies ongoing.
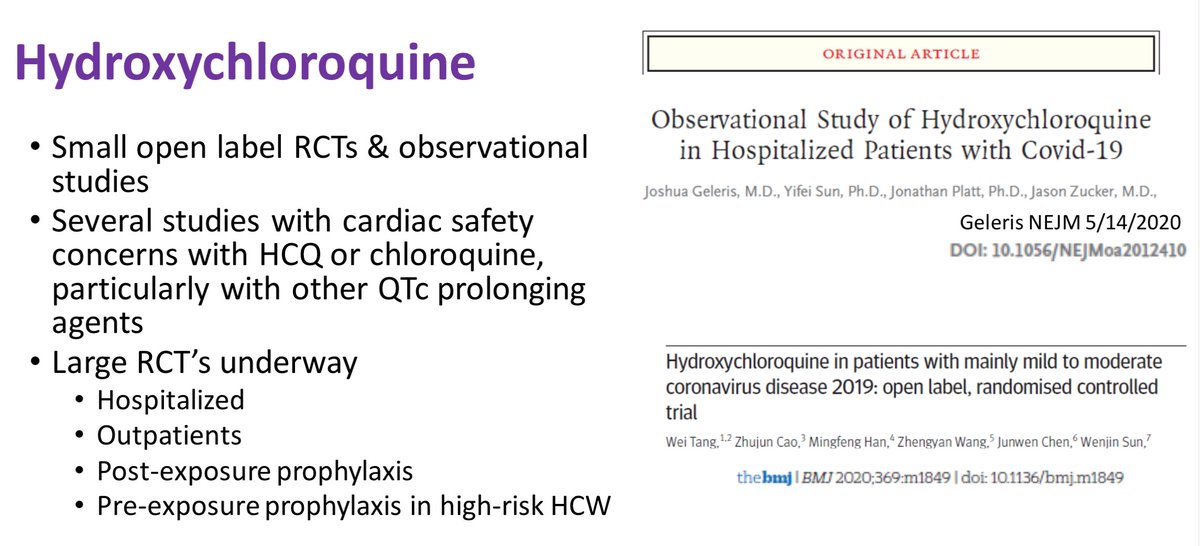
17/ @ 37:35: Hydroxychloroquine: disappointing results to date. @ 44:22: I pushed Annie on whether we’d have shelved the drug by now if it wasn’t being pushed by Trump. She was equivocal, but agreed that – while there was some promise early – there is little to commend it now.
18/ Next, @ 46:42, vaccines w/ Joel Ernst. I had chatted w/ Joel on Mon bit.ly/3c0ba0V re @moderna_tx's early results. His new insights today: @ 48:50, while 8 out of 45 pts had neutralizing antibodies, he clarifies that others weren’t neg; they haven’t been reported yet
19/ @ 52:20: The @moderna_tx is RNA vaccine: there’s no RNA vaccine in use today (it’s based on v. modern technology). This increases risk that there'll be a surprise problem.
@ 53:10, next step in testing Moderna vaccine is expanding safety trial to 600 pts, incl. pts >age 55
@ 53:10, next step in testing Moderna vaccine is expanding safety trial to 600 pts, incl. pts >age 55
20/ @ 56:00, Joel gives more details on the two ways of testing vaccine efficacy: a population-based study vs. a human challenge. He also notes that some vaccines block infections; other effective vaccines just attenuate the illness rather than completely blocking infection.
21/ @ 1:01;05: even if everything goes perfectly in further tests of @moderna_tx vaccine, Ernst thinks we’re still at least a year away from routine availability for high-risk populations. And, to produce billions of doses for everybody, add some time on time on top of that.
22/ Final topic, @ 1:03:00, Andy Leavitt on thromboembolic complications (aka “Covid-Associated Coagulopathy”). It’s the real deal, and “we don’t understand it mechanistically.” It’s not just a form of DIC (a fairly common bleeding/clotting abnormality in very sick patients).
23/ @ 1:13:30, in French study of 150 pts, 64 had significant thrombosis, even though all were getting VTE prophylaxis.. This is astounding. Most amazing: high rate (96%) of clotting the circuit when patients were getting renal support; this is simply not seen in other diseases.
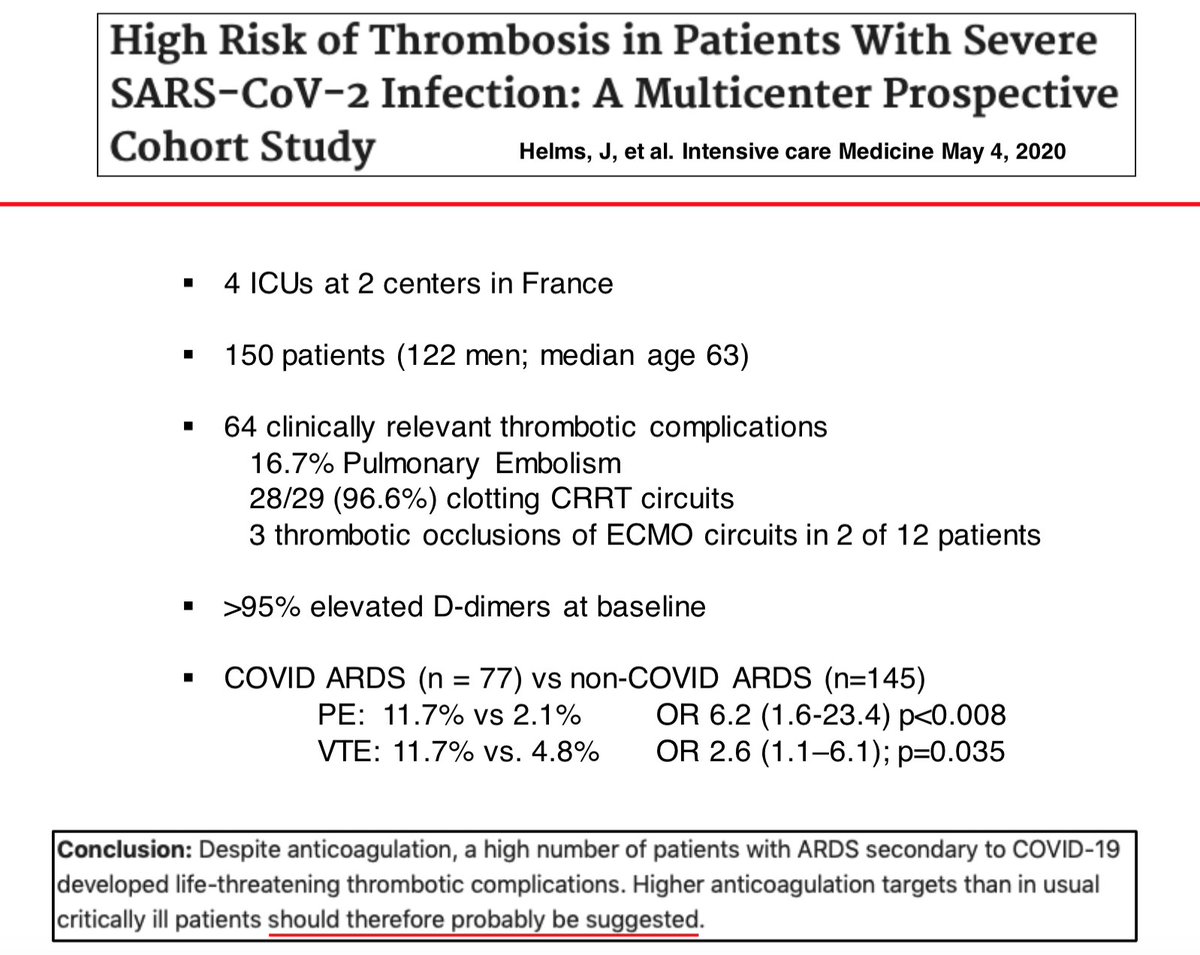
24/ @ 1:20:00, Leavitt recommends higher dose of anticoagulation than usual, but doesn’t recommend therapeutic-dose anticoag for Covid pt without clot. Nor would he recommend anticog or aspirin for outpatients with Covid. The clots are scary, but anticoagulation is risky as well.
25/ Another great grand rounds; watch if you can bit.ly/3bTcpP9. Clinically, Covid is wild. Kids don’t get too sick (good), but now there's MIS-C (bad). & bizarre clots. Covid is relentless teacher of clinical medicine. And it's not the flu.
Back tomorrow. Stay safe.
Back tomorrow. Stay safe.