
Dual-Energy CT to Differentiate Small Foci of Hemorrhage From Calcium
A #TWEETORIAL for #RadRes and #MedStudentTwitter
Inspired by the recent @radiology_rsna article: pubs.rsna.org/doi/10.1148/ra…
Important work from our very own @BWHRadEdu @walterfwiggins @AaronSodickson
A #TWEETORIAL for #RadRes and #MedStudentTwitter
Inspired by the recent @radiology_rsna article: pubs.rsna.org/doi/10.1148/ra…
Important work from our very own @BWHRadEdu @walterfwiggins @AaronSodickson
2/
First some background:
Non-contrast Head CT is the first-line imaging study in trauma.
While most acute hemorrhage can be diagnosed confidently on a CT, small foci of hemorrhage and calcification can be hard to differentiate. This is where dual-energy CT (DECT) can help!
First some background:
Non-contrast Head CT is the first-line imaging study in trauma.
While most acute hemorrhage can be diagnosed confidently on a CT, small foci of hemorrhage and calcification can be hard to differentiate. This is where dual-energy CT (DECT) can help!
3/
To understand DECT, we have to understand some basic CT physics concepts.
POLL: In diagnostic imaging, photon absorption for high atomic number elements is dominated by what process?
A) Photoelectric effect
B) Compton scattering
C) Rayleigh scattering
D) Pair production
To understand DECT, we have to understand some basic CT physics concepts.
POLL: In diagnostic imaging, photon absorption for high atomic number elements is dominated by what process?
A) Photoelectric effect
B) Compton scattering
C) Rayleigh scattering
D) Pair production
4/
The photoelectric absorption is related to its atomic number and k edge, which reflects the energy level of the atom’s innermost electron k-shell.
Elements which have a higher atomic number will have a higher-energy k shells and hence a higher k edge.
The photoelectric absorption is related to its atomic number and k edge, which reflects the energy level of the atom’s innermost electron k-shell.
Elements which have a higher atomic number will have a higher-energy k shells and hence a higher k edge.

5/
In DECT, x-ray absorption data are gathered from low- and high-energy x-ray spectra to capitalize on the differences in energy-dependent x-ray absorption of different materials.
For example, the mean x-ray energy for a typical 120-kV spectrum is 70 keV.
In DECT, x-ray absorption data are gathered from low- and high-energy x-ray spectra to capitalize on the differences in energy-dependent x-ray absorption of different materials.
For example, the mean x-ray energy for a typical 120-kV spectrum is 70 keV.
6/
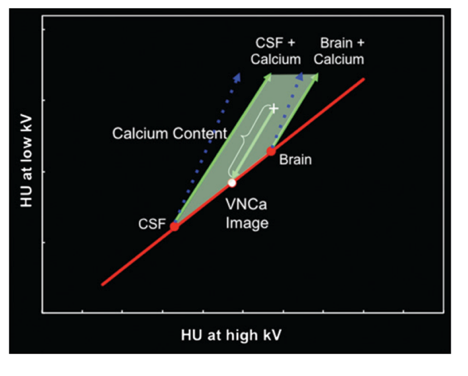
Since the K edge of Calcium is 4 keV, Ca will result in GREATER increases in attenuation at LOWER kV settings, giving rise to a characteristic slope. A three-material decomposition can be done to separate the component of Ca in every voxel.
Fig from:
pubs.rsna.org/doi/10.1148/rg…
Since the K edge of Calcium is 4 keV, Ca will result in GREATER increases in attenuation at LOWER kV settings, giving rise to a characteristic slope. A three-material decomposition can be done to separate the component of Ca in every voxel.
Fig from:
pubs.rsna.org/doi/10.1148/rg…
7/
Getting back to the study… the PURPOSE: Quantify the diagnostic performance of DECT versus simulated single-energy CT in the differentiation of small foci of ICH from calcium.
Getting back to the study… the PURPOSE: Quantify the diagnostic performance of DECT versus simulated single-energy CT in the differentiation of small foci of ICH from calcium.
8/
MATERIAL & METHOD
467 consecutive dual-energy unenhanced CTs of the head performed at the @BWHRadiology ED were included if:
1) Hyperattenuating foci > 100 HU
2) Minimum focus diameter > 2.5 mm
3) Binary classification of Ca vs. Hemorrhage was possible.
MATERIAL & METHOD
467 consecutive dual-energy unenhanced CTs of the head performed at the @BWHRadiology ED were included if:
1) Hyperattenuating foci > 100 HU
2) Minimum focus diameter > 2.5 mm
3) Binary classification of Ca vs. Hemorrhage was possible.
9/
MATERIAL & METHOD CONTD
All of the single-energy CT scans were read by a #radres and each was classified as:
1) CONFIDENT calcification
2) CONFIDENT hemorrhag
3) INDETERMINATE
MATERIAL & METHOD CONTD
All of the single-energy CT scans were read by a #radres and each was classified as:
1) CONFIDENT calcification
2) CONFIDENT hemorrhag
3) INDETERMINATE
10/
REFERENCE TRUTH characterization was made by comparing with a follow-up CT or MRI.
It was classified as HEMORRHAGE:
a) If it was new from 1 month prior
AND IF
b) Perilesional edema on a follow-up image or MRI demonstrated phase signal consistent with blood on SWI
REFERENCE TRUTH characterization was made by comparing with a follow-up CT or MRI.
It was classified as HEMORRHAGE:
a) If it was new from 1 month prior
AND IF
b) Perilesional edema on a follow-up image or MRI demonstrated phase signal consistent with blood on SWI
11/
It was classified as CALCIUM:
a) No morphologic features to suggest alternative diagnosis
AND
b) Unchanged from a prior at least 1 month before or after the study or if MRI demonstrated phase signal opposite to blood pool on SWI
It was classified as CALCIUM:
a) No morphologic features to suggest alternative diagnosis
AND
b) Unchanged from a prior at least 1 month before or after the study or if MRI demonstrated phase signal opposite to blood pool on SWI
12/
The initial assessment made by the #radres was therefore determined as CONCORDANT or DISCORDANT based on comparison with the reference truth.
Hyperattenuating foci were divided into:
A development set of foci, all with CONFIDENT assessment and which were CONCORDANT
The initial assessment made by the #radres was therefore determined as CONCORDANT or DISCORDANT based on comparison with the reference truth.
Hyperattenuating foci were divided into:
A development set of foci, all with CONFIDENT assessment and which were CONCORDANT
13/
AND
Test set of foci which were either INDETERMINATE on initial assessment or with DISCORDANT reference truths.
AND
Test set of foci which were either INDETERMINATE on initial assessment or with DISCORDANT reference truths.
14/
Quantitative analysis was performed by the #radres placing an ROI centered on the highest attenuation component and recording:
1) Single-energy CT attenuation
2) Calculated attenuation of the VNCa (virtual non-Ca) component
3) Calculated attenuation of the Ca component
Quantitative analysis was performed by the #radres placing an ROI centered on the highest attenuation component and recording:
1) Single-energy CT attenuation
2) Calculated attenuation of the VNCa (virtual non-Ca) component
3) Calculated attenuation of the Ca component
15/
The test set was used in a blinded reader study with 2 expert ED Radiologists. In each of the phases, a focus was classified based on the Likert scale as follows:
-2Certain Calcium
-1Likely Calcium
0Uncertain
1Likely Hemorrhage
2Certain Hemorrhage
The test set was used in a blinded reader study with 2 expert ED Radiologists. In each of the phases, a focus was classified based on the Likert scale as follows:
-2Certain Calcium
-1Likely Calcium
0Uncertain
1Likely Hemorrhage
2Certain Hemorrhage
16/
PH 1: Readers evaluated the single-energy CT images
PH 2: Readers qualitatively assessed axial VNCa and Ca overlay images
PH 3: Readers placed DE ROIs within the focus and compared attenuation against proposed thresholds
(VNCa as subplot B and Ca overlay as subplot C)
PH 1: Readers evaluated the single-energy CT images
PH 2: Readers qualitatively assessed axial VNCa and Ca overlay images
PH 3: Readers placed DE ROIs within the focus and compared attenuation against proposed thresholds
(VNCa as subplot B and Ca overlay as subplot C)

17/
RESULTS
Candidate CT attenuation thresholds were derived from the development set by using univariable and bivariate logistic regression and maximizing the F1 score (harmonic average of sensitivity and PPV).
RESULTS
Candidate CT attenuation thresholds were derived from the development set by using univariable and bivariate logistic regression and maximizing the F1 score (harmonic average of sensitivity and PPV).

18/
RESULTS CONTD
Using the derived thresholds on the VNCa component and Ca component on the test set improved accuracy to 95% from 49% when compared to using a threshold on the single-energy CT.
RESULTS CONTD
Using the derived thresholds on the VNCa component and Ca component on the test set improved accuracy to 95% from 49% when compared to using a threshold on the single-energy CT.

19/
The AUC (area under the curve) from a ROC analysis demonstrates increased performance of both readers in phase 2 (qualitative eval of the VNCa and Ca overlay) (as solid lines) in comparison to phase 1 (using single energy CT) (dotted lines).
The AUC (area under the curve) from a ROC analysis demonstrates increased performance of both readers in phase 2 (qualitative eval of the VNCa and Ca overlay) (as solid lines) in comparison to phase 1 (using single energy CT) (dotted lines).

20/
RESULTS CONTD
Dual-energy CT increased diagnostic confidence (classifications rated as “certain”) from 71% to 90% for Reader 1 and from 46% to 85% for Reader 2 in comparison to the single-energy.
RESULTS CONTD
Dual-energy CT increased diagnostic confidence (classifications rated as “certain”) from 71% to 90% for Reader 1 and from 46% to 85% for Reader 2 in comparison to the single-energy.

21/
IN SUMMARY
Dual-energy CT showed high diagnostic performance in the differentiation of small foci of intracranial hemorrhage from calcium and improved diagnostic accuracy and confidence in evaluation of suspected hemorrhage.
IN SUMMARY
Dual-energy CT showed high diagnostic performance in the differentiation of small foci of intracranial hemorrhage from calcium and improved diagnostic accuracy and confidence in evaluation of suspected hemorrhage.
@threadreaderapp
unroll
unroll

