[thread] The paradox of treating ARDS is this: because we don't have a drug to reverse lung injury, we provide supportive care with two therapies - oxygen and mechanical ventilation - that can both cause ARDS.
Like treating cancer w/ carcinogens. Or infections w/ pathogens.
1/n
Like treating cancer w/ carcinogens. Or infections w/ pathogens.
1/n
We've known that oxygen causes lung injury for 250 years. Lavoisier stuck guinea pigs in "l'air vital" and watched them die from "une fièvre ardente" and a "maladie inflammatoire." Their lungs were flacid, red, and engorged with blood. Their right ventricles were dilated.
2/n
2/n
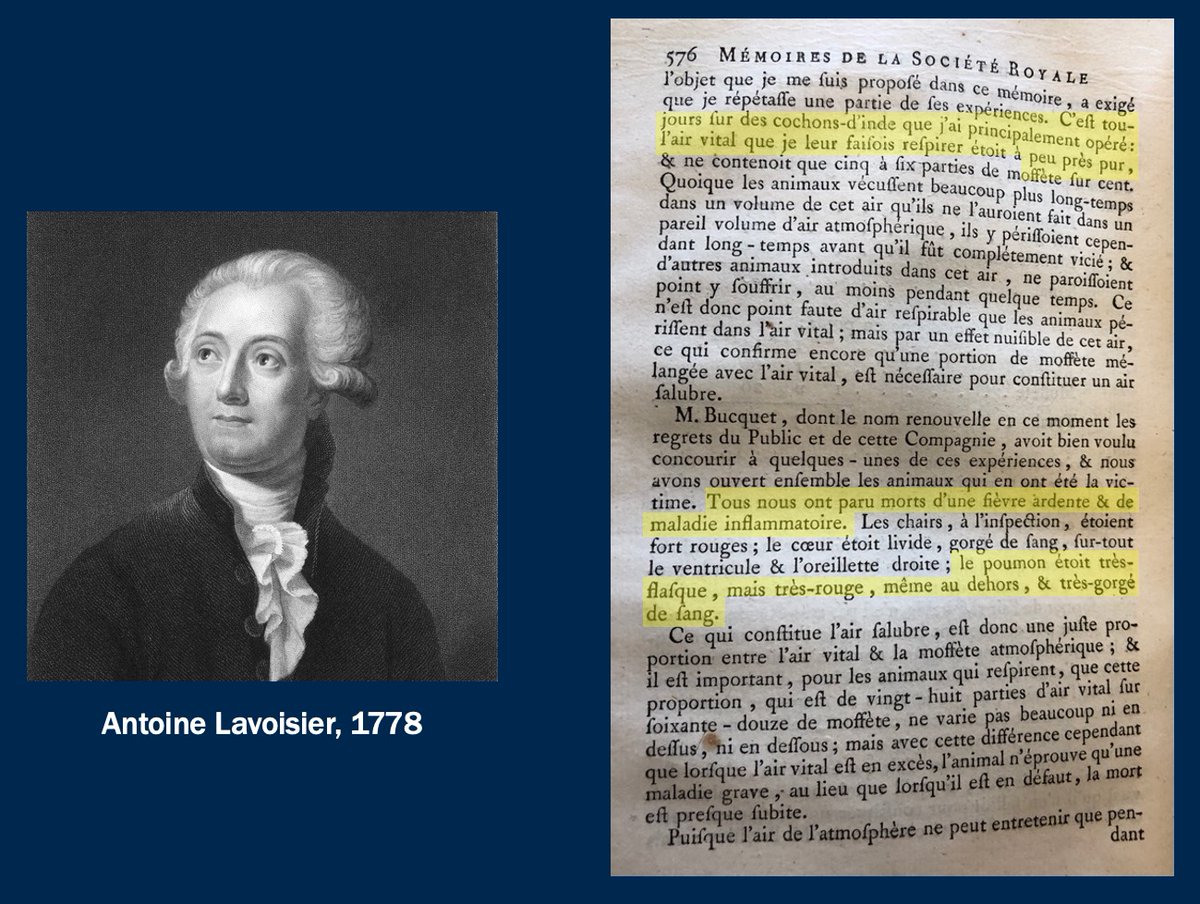
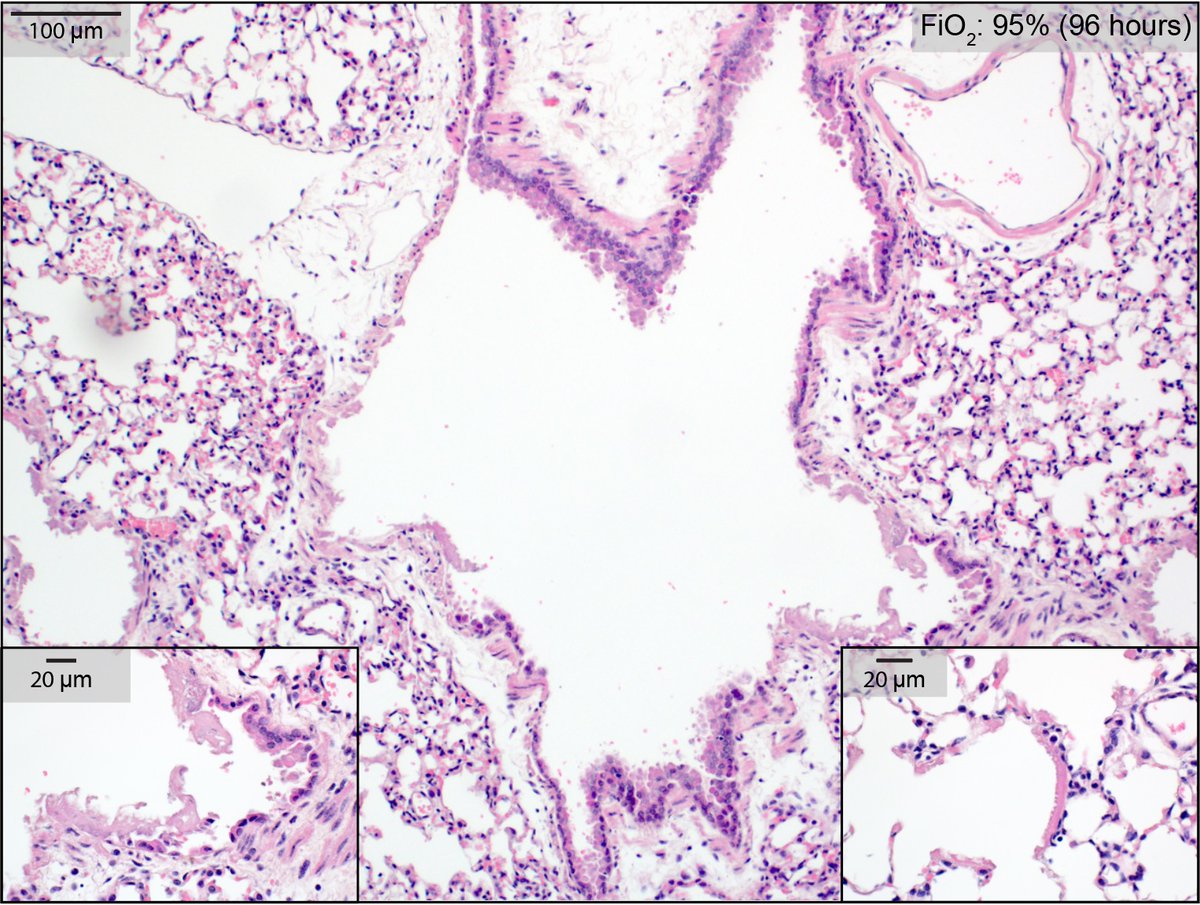
He was describing ARDS (w/ cor pulmonale), 200 years before we named it. If he'd had microscopy, he'd have seen epithelial necrosis, hyaline membranes: diffuse alveolar damage. Same injury pattern that COVID causes. (Image from my lab: healthy mouse, 95% FiO2 for 4 days.)
3/n
3/n
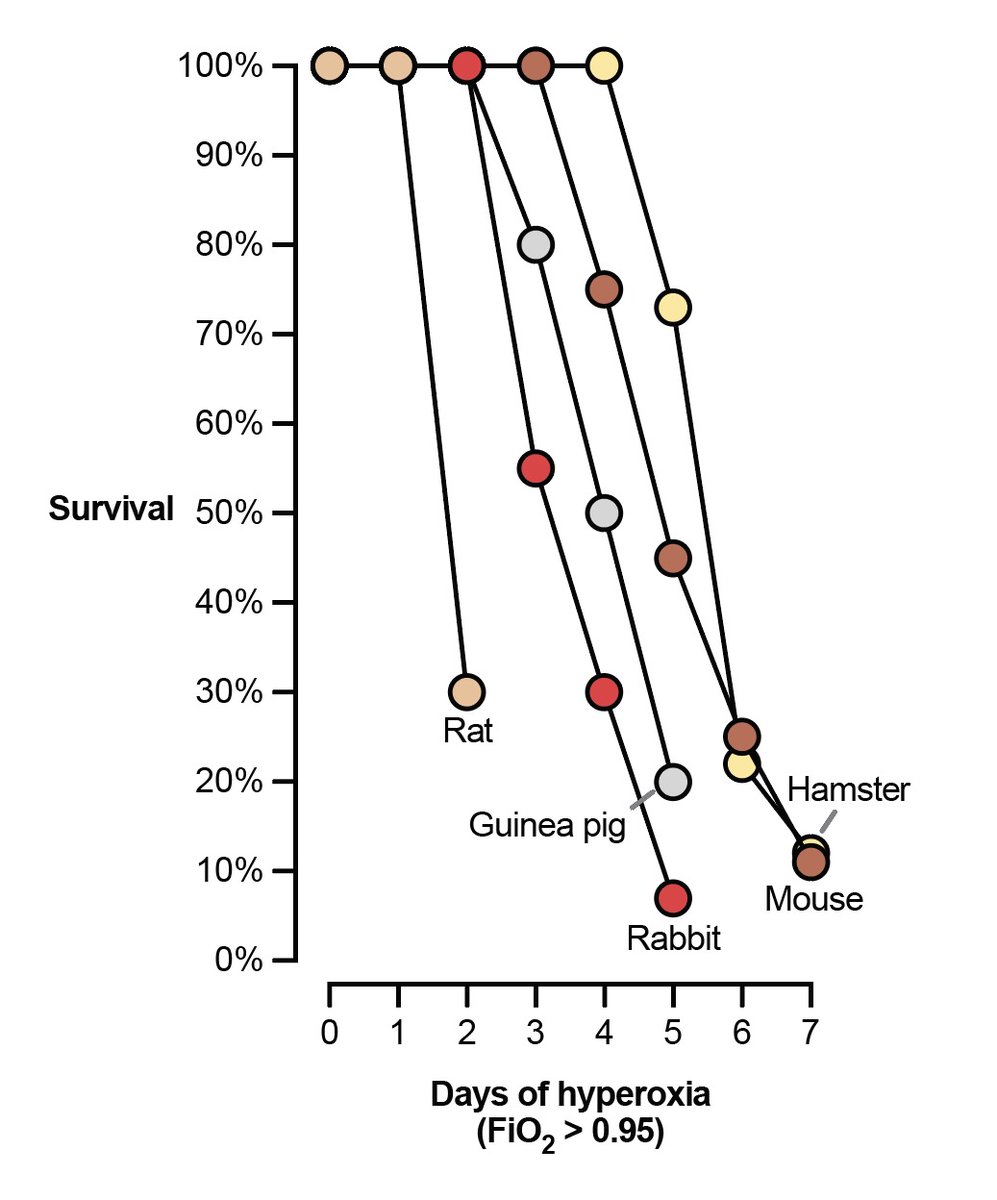
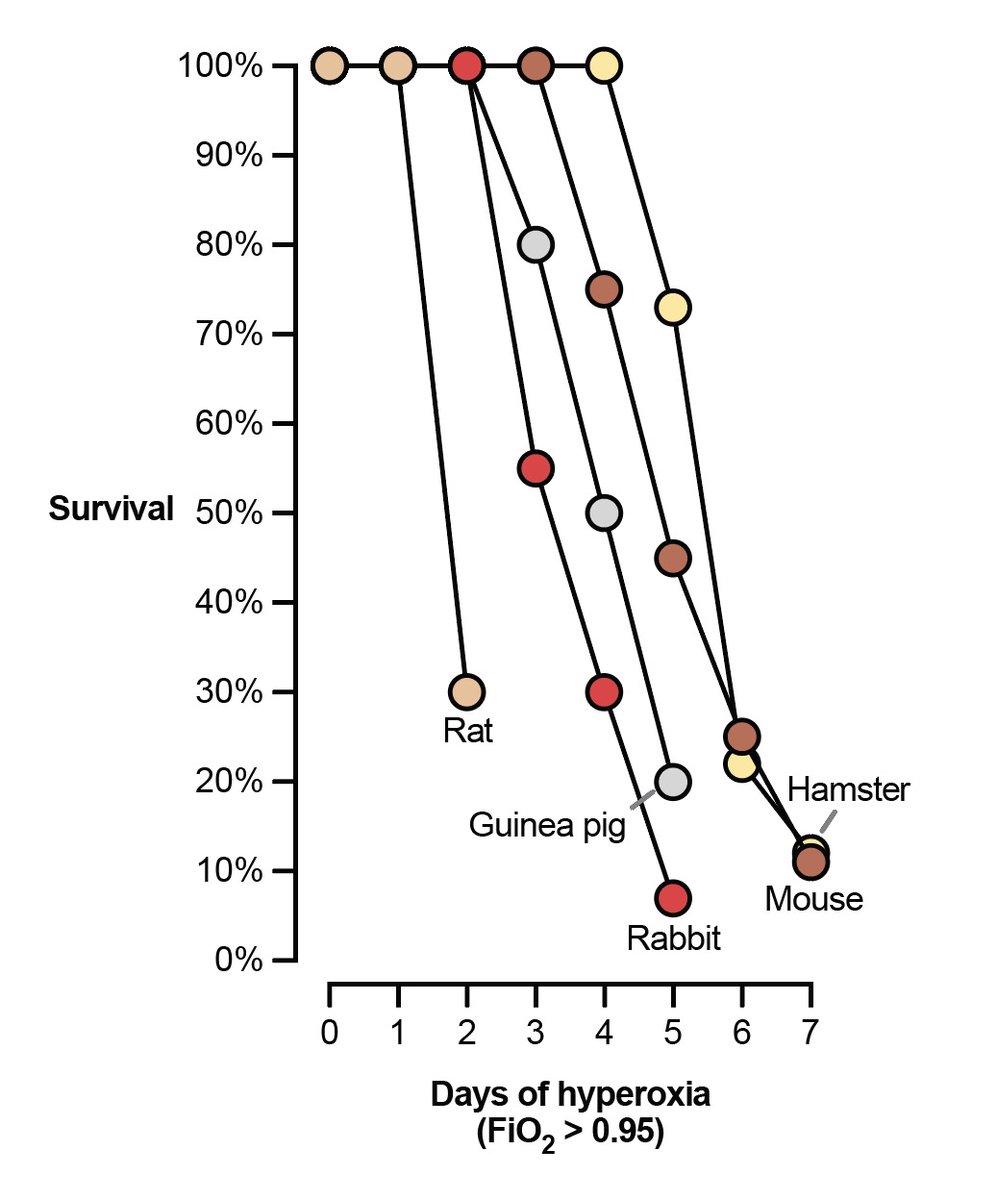
This observation (O2 --> ARDS) is universal among animals with lungs. If you give mammal pure oxygen to breathe, it'll die within a week with severe lung injury.
(Figure adapted from ncbi.nlm.nih.gov/pubmed/730565)
4/n
(Figure adapted from ncbi.nlm.nih.gov/pubmed/730565)
4/n
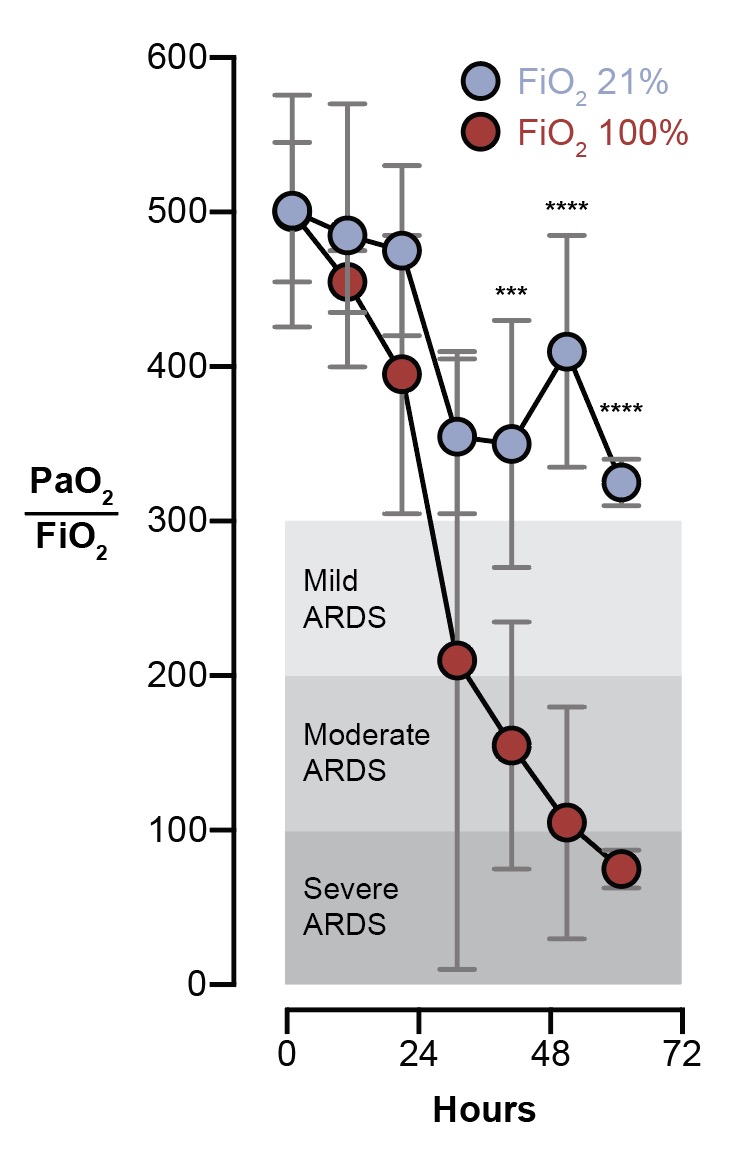
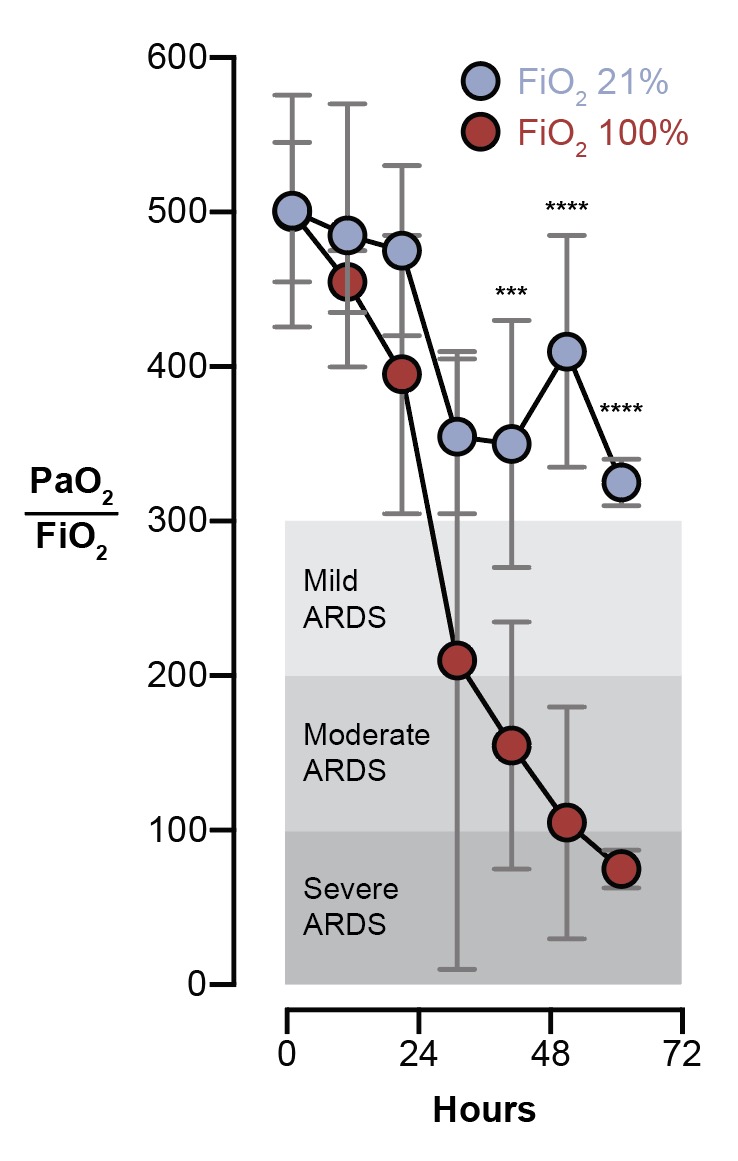
Humans are not an exception. If you take a group of brain dead patients and give half of them 100% FiO2, they'll have severe hypoxic respiratory failure within 3 days. The control group (21% FiO2) will not.
(Figure adapted from ncbi.nlm.nih.gov/pubmed/4921729)
5/n
(Figure adapted from ncbi.nlm.nih.gov/pubmed/4921729)
5/n
For all the bad press that mechanical ventilation has gotten recently, I worry what will happen when the word gets out about oxygen. It's pretty toxic for lungs!
6/n
6/n
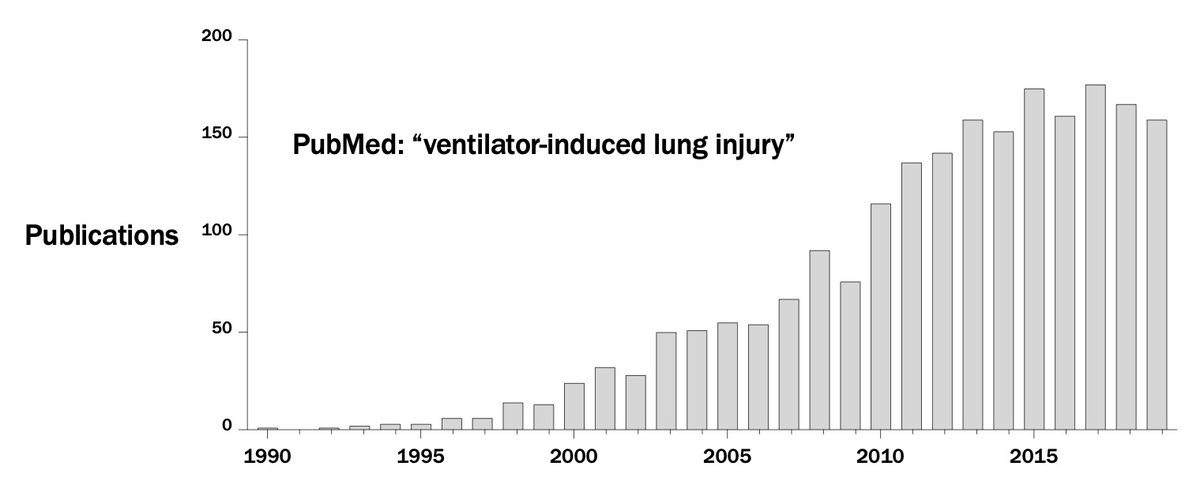
And while you might get the impression that "some doctors" and Elon Musk have recently discovered the danger of ventilators, this has been a topic of intense study for 30 years. It is unambiguous that mechanical ventilation can cause... ARDS.
7/n
7/n
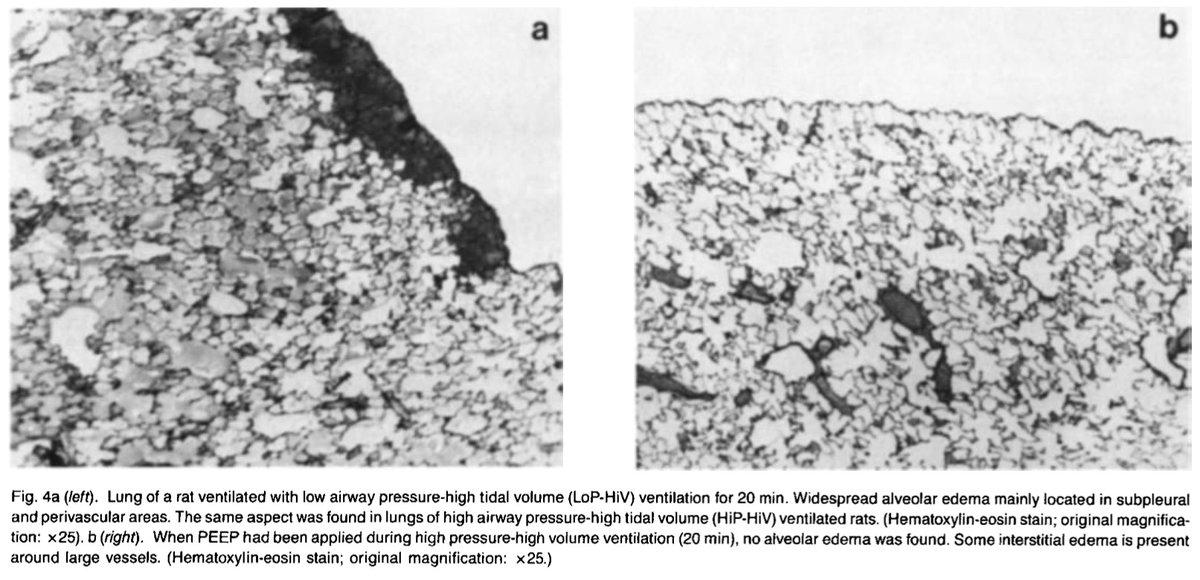
If you ventilate healthy animals with high pressures (w/ a vent) or high volumes (w/ an iron lung), you cause... diffuse alveolar damage. Again, the same pattern of injury we see in COVID lungs. Ventilators can cause ARDS.
(Image from ncbi.nlm.nih.gov/pubmed/3057957... 1988!)
8/n
(Image from ncbi.nlm.nih.gov/pubmed/3057957... 1988!)
8/n
So this is our challenge: in a patient with severe lung injury causing hypoxemia, our only options are 1) give them oxygen, which can cause ARDS; 2) mechanically ventilate them, which can cause ARDS; or 3) tolerate hypoxemia. That's a tough choice! We don't make it lightly.
9/n
9/n
Our imperfect solution is to use a combination of all three to minimize harm from any one of them. Tolerate lower-than-normal-but-not-life-threatening blood oxygen levels. Give just enough O2 and mechanical ventilation to support the patient without worsening the problem.
10/n
10/n
All of our effective therapies are basically harm reduction strategies. PEEP is an FiO2-sparing intervention. Lung-protective ventilation, neuromuscular blockade, and proning are all meant to reduce the violence we do to lungs with the ventilator.
11/n
11/n
Think of O2 and the ventilator like you think of a scalpel. It's a murder weapon, but if used sparingly and judiciously, it can save lives.
12/n
12/n
But UNLIKE with scalpels, we can't immediately tell that we're hurting patients with O2 and vents. My mice in 95% oxygen look great! You'd never know by looking at them that they are 3-4 days away from severe ARDS.
13/n
13/n
Likewise with vents. Patients might look _better_ (in terms of oxygenation, comfort, etc.) with settings that worsen lung injury (e.g. the control arm in ARMA that didn't receive LPV).
You just can't tell by looking at a patient if your intervention is hurting them.
14/n
You just can't tell by looking at a patient if your intervention is hurting them.
14/n
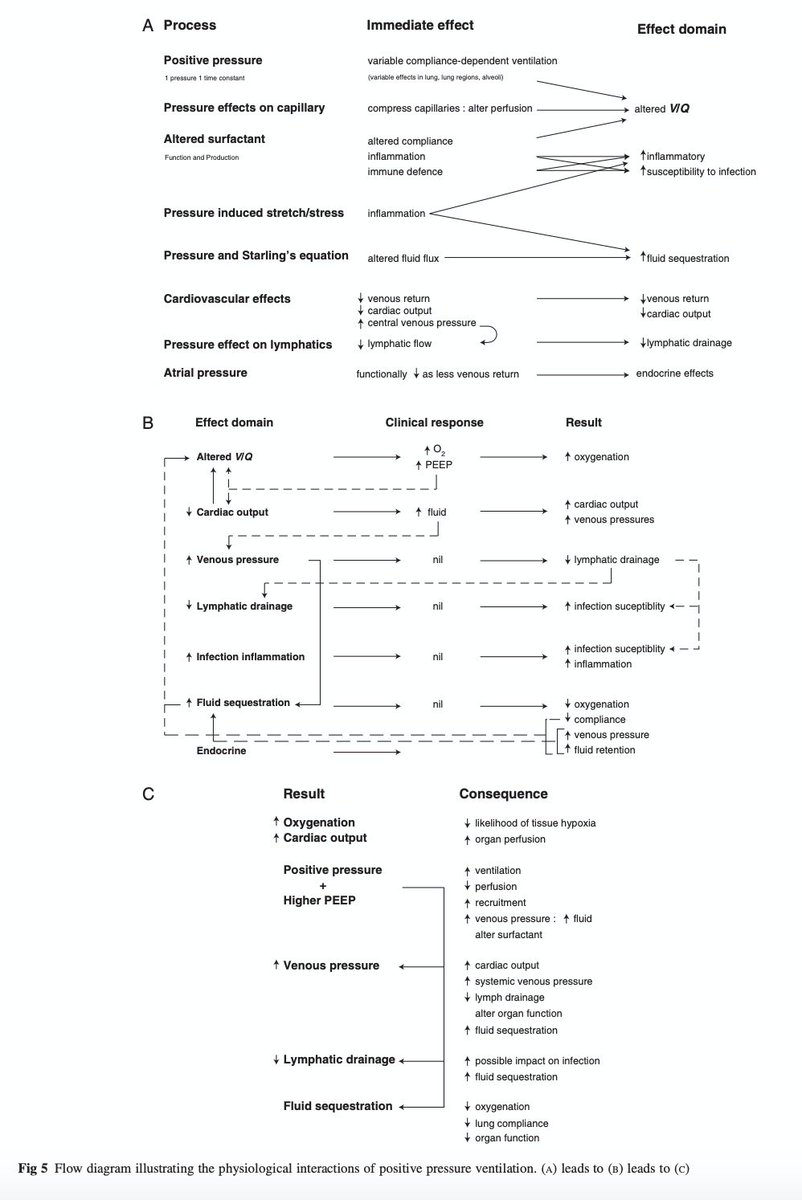
Every change we make on the vent has a cascade of effects across organ systems: not merely (merely!) pulmonary and cardiac, but also lymphatics, inflammation & coagulation, renal...
We should be humble when predicting effects of our interventions.
academic.oup.com/bja/article/10…
15/n
We should be humble when predicting effects of our interventions.
academic.oup.com/bja/article/10…
15/n
So when someone suggests we 'keep COVID patients off vents,' I need to know the opportunity costs.
Are you ok with very high doses of O2 for days? As in, literally my animal model of ARDS? Are you sure that's better for patients than lower FiO2 with a modest PEEP setting?
16/n
Are you ok with very high doses of O2 for days? As in, literally my animal model of ARDS? Are you sure that's better for patients than lower FiO2 with a modest PEEP setting?
16/n
Embracing the theme of humility: I don't profess to know the optimal balance of harms caused by hypoxemia, O2 toxicity, and VILI.
But I know that as a field, we've made steady, incremental progress in improving ARDS outcomes in recent decades. We're getting better at it.
17/n
But I know that as a field, we've made steady, incremental progress in improving ARDS outcomes in recent decades. We're getting better at it.
17/n
And we are studying the hell out of these things. E.g. this month a 40K patient study of O2 targeting was launched that will make us smarter about minimizing O2 harm (@DogICUma). We constantly strive to innovate and improve our vent management.
18/n
18/n
One day we'll have drugs that restore lung function and our current measures will seem primitive. It'll be great! But until then, we're working with what we've got: saving lives of people with ARDS using tools that cause ARDS while trying not to cause more ARDS.
19/19
19/19