#ASCO20 The RAMES study was a phase II trial of 2nd line gemcitabine +/- ramucirumab for pleural mesothelioma (#MPM). VEGF is an enticing target. MAPS showed adding bev to cis/pem improved OS (not FDA approved) though LUME-meso (nintedanib + cis/pem) was negative. #OncoAlert 
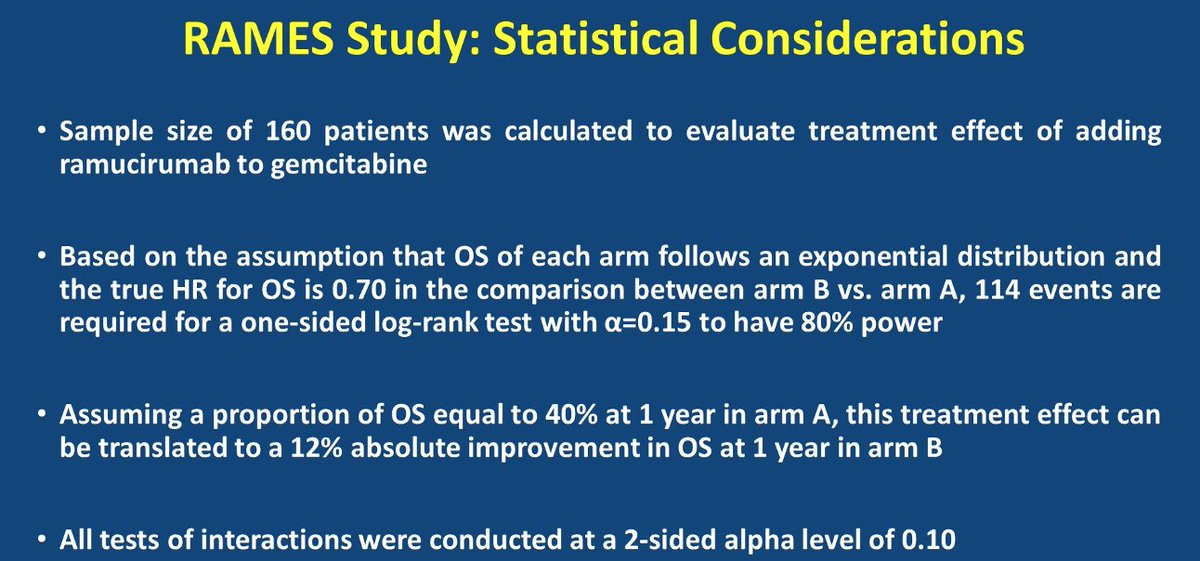
#ASCO20 RAMES was a 1:1 randomization of gem 1000mg/m2 d1/8 with or without ram 10mg/kg in 21d cycles. Primary endpoint was OS. Included MPM with PD after platinum/pemetrexed. Treated 161 patients, 85% epithelioid. #OncoAlert


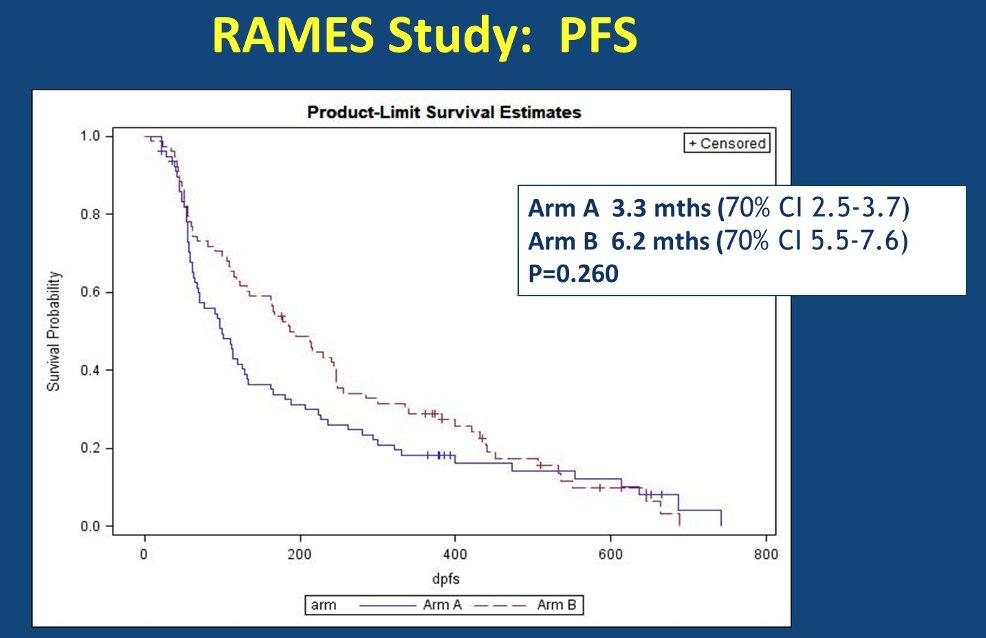
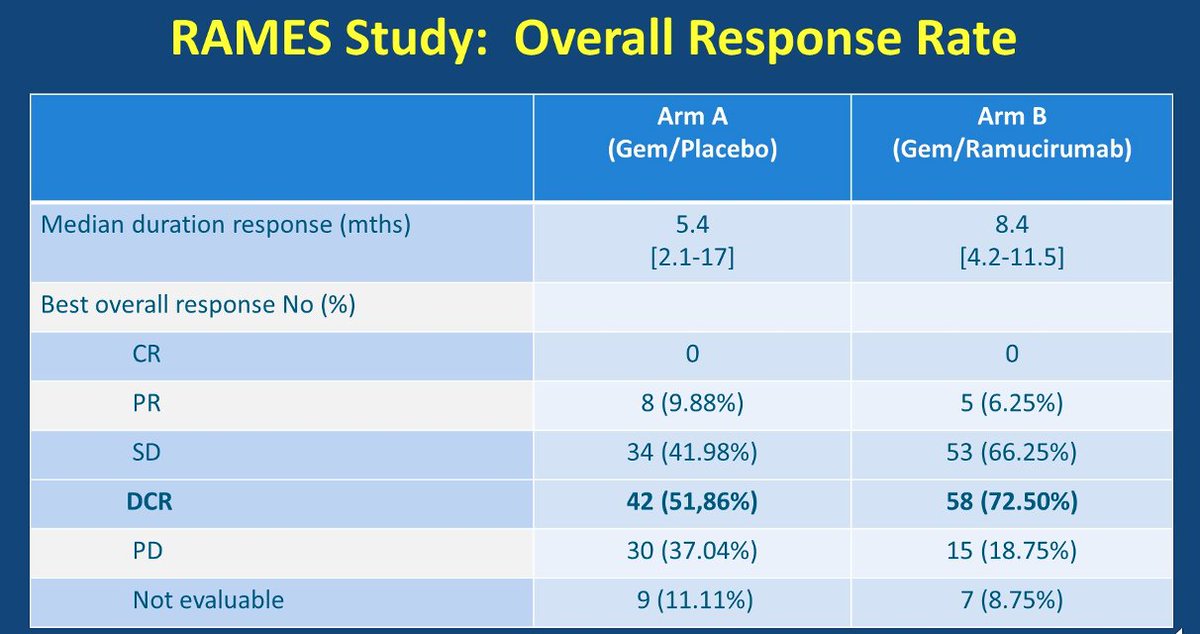
#ASCO20 Addition of ramucirumab to 2nd line gemcitabine improved OS in #MPM. Median from 7.5m to 13.8m (HR 0.71). 1y OS rate 34% to 57%. PFS numerically better (3.3m to 6.2m, p=0.26). Note that RR not higher, mostly SD. The benefit is survival. #OncoAlert


#ASCO20 G3+ toxicity rates relatively low with addition of ramucirumab, though class toxicities were seen (HTN, thromboembolism, proteinuria). QOL studies ongoing. Supports VEGFR2 as a target for #MPM. #OncoAlert

• • •
Missing some Tweet in this thread? You can try to
force a refresh