#ASCO20 A lot to think about with the data from the #SINDAS trial: a randomized phase 3 trial of early local radiation therapy for patients with metastatic #EGFR mutant #NSCLC presented by Dr. Xiao-Shan Wang. #OncoAlert #LCSM 
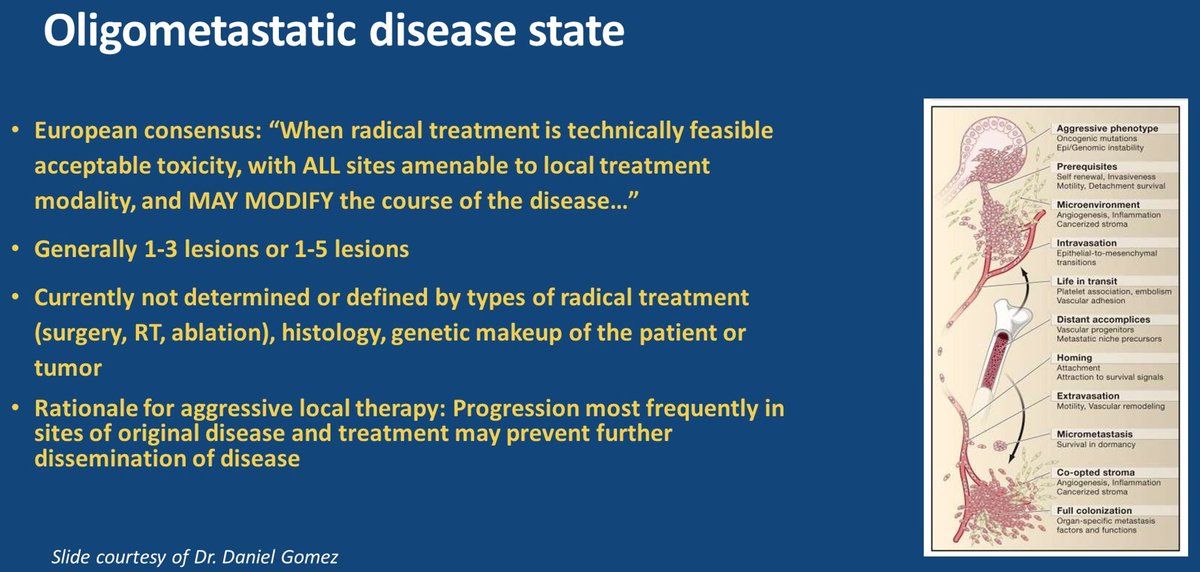
#ASCO20 At this point, we're on board with the concept of oligometastatic NSCLC - that there is a spectrum within stage IV lung cancer and aggressive therapy for some will improve outcomes. Various definitions (would a biologic marker be better than # of radiographic lesions?)


#ASCO20 SINDAS enrolled 133pts with oligometastatic #EGFR NSCLC, defined as up to 5 metastases (max of 2 per organ), EXCLUDING brain metastases, ECOG 0-2. Used a 1:1 randomization to SBRT + TKI vs TKI alone, PFS primary endpoint. #OncoAlert #LCSM
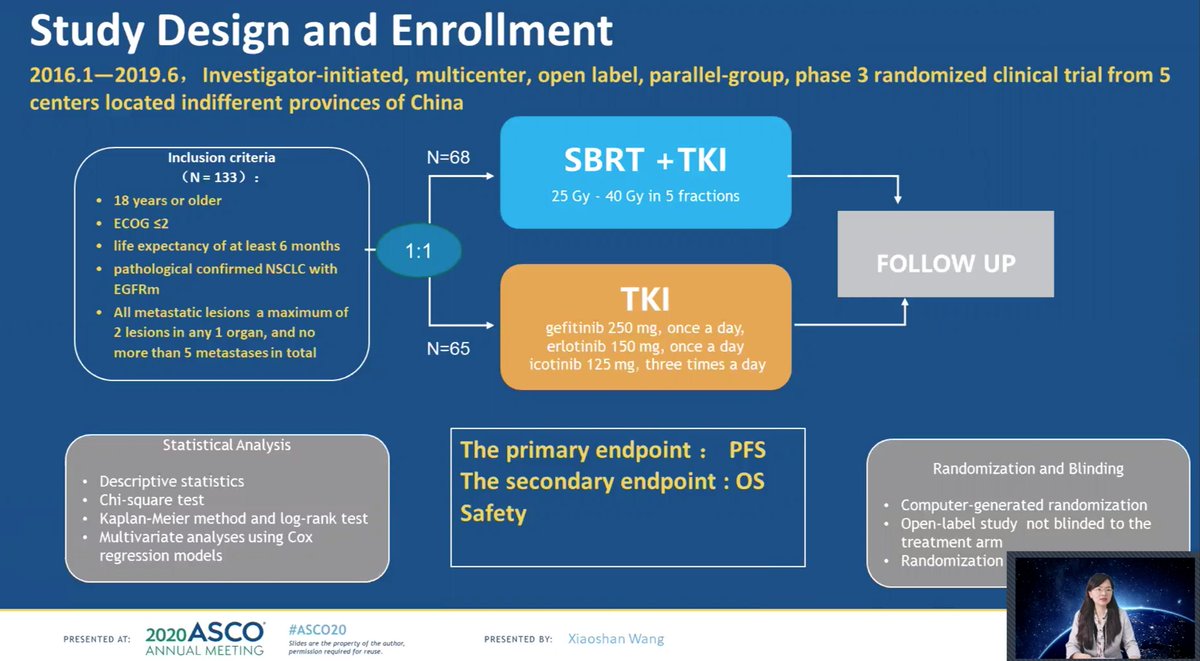
#ASCO20 One of the limitations is generalizability. Screened 631 patients over 3+ years to enroll 136 patients (78% screen fail). Included EGFR exon 20 insertions (and unbalanced between arms) and only used first generation EGFR TKIs. And again, excluded pts with brain metastases


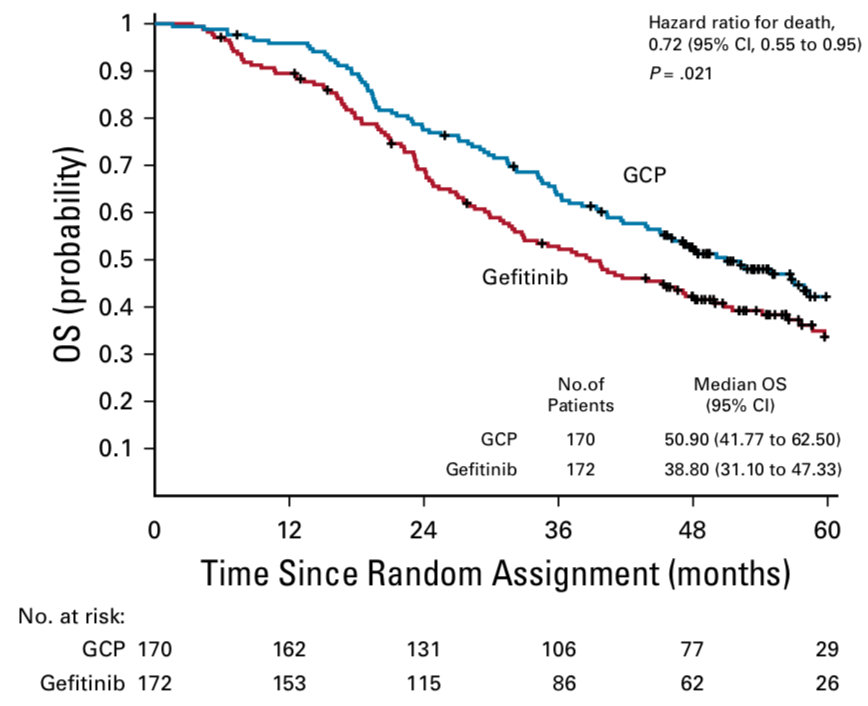
#ASCO20 Despite limitations, the impact was notable. Upfront SBRT improved PFS (HR 0.618) and OS (HR 0.682). Similar toxicity except pneumonitis was more common with SBRT (the 30% in the table seems to describe fraction of all G3 events and not % of pts, for some reason). #LCSM




#ASCO20 Benefit of upfront SBRT was significant. The absolute numbers have little meaning to me due to the population (no CNS mets, some EGFRex20) and subsequent therapy (no osi used, only chemo as salvage) and need more complete data on toxicity. But the strategy is logical.

#ASCO20 Known OS benefit with addition of chemotherapy to #EGFR TKI, presumably targeting clones that persist despite TKI. SBRT is another, non-cross resistant means to do that. Could we do chemo+TKI with SBRT to persistent lesions? Will more aggressive 1L tx stave of resistance?

• • •
Missing some Tweet in this thread? You can try to
force a refresh