1/ Covid (@UCSF) Chronicles, Day 83
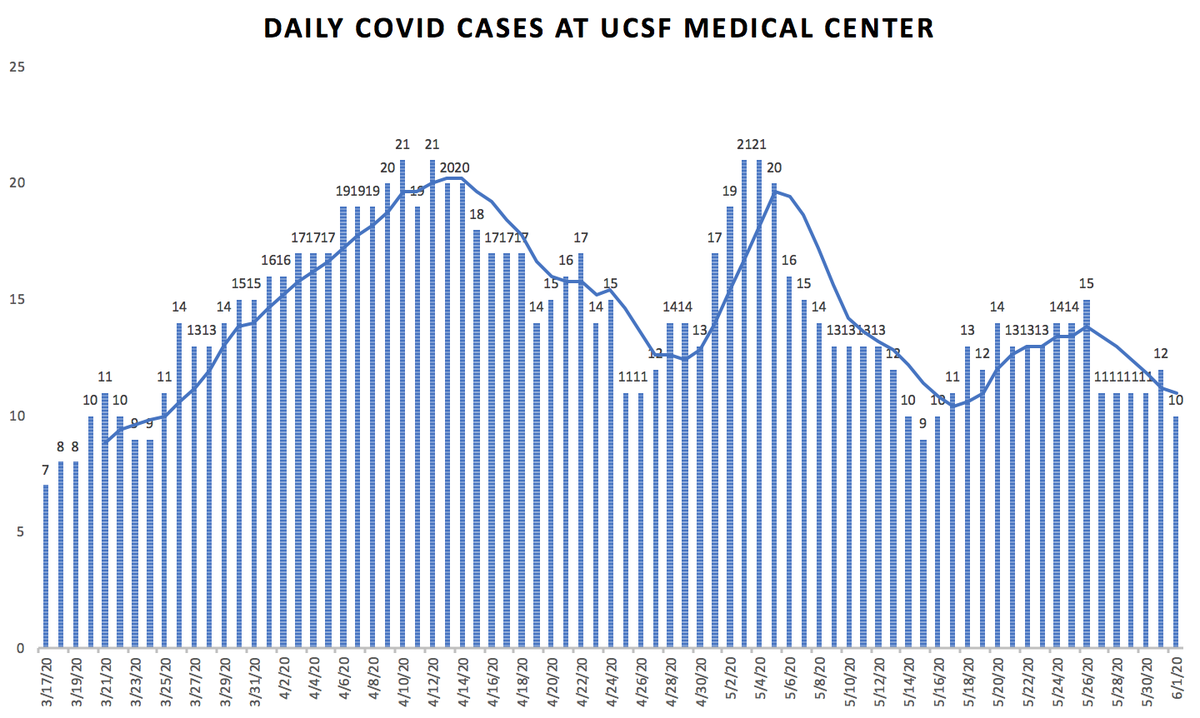
@ucsfhospitals, 10 pts, 2 on vents: fewest vented pts we’ve had since March.
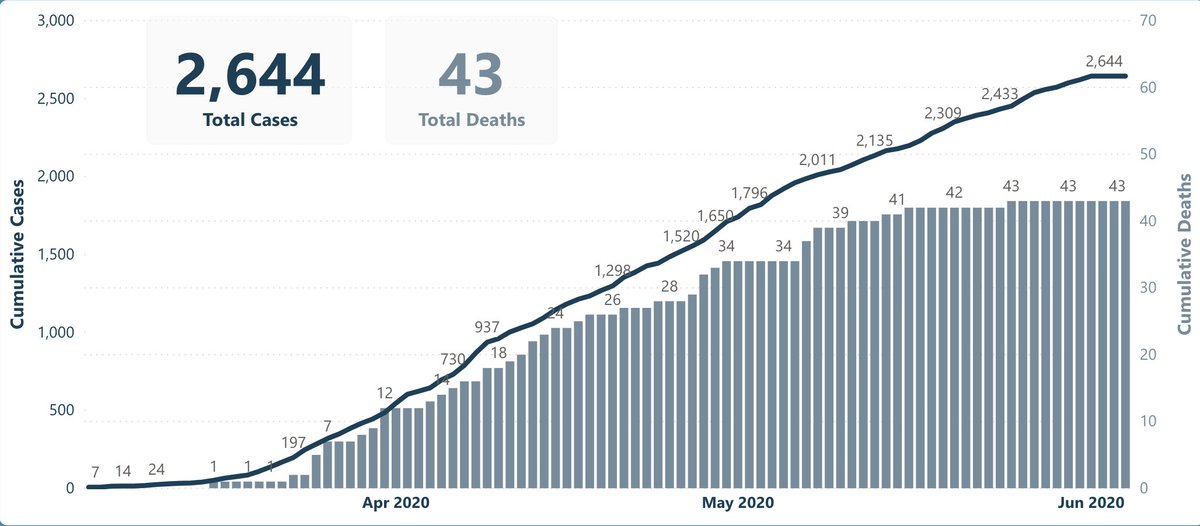
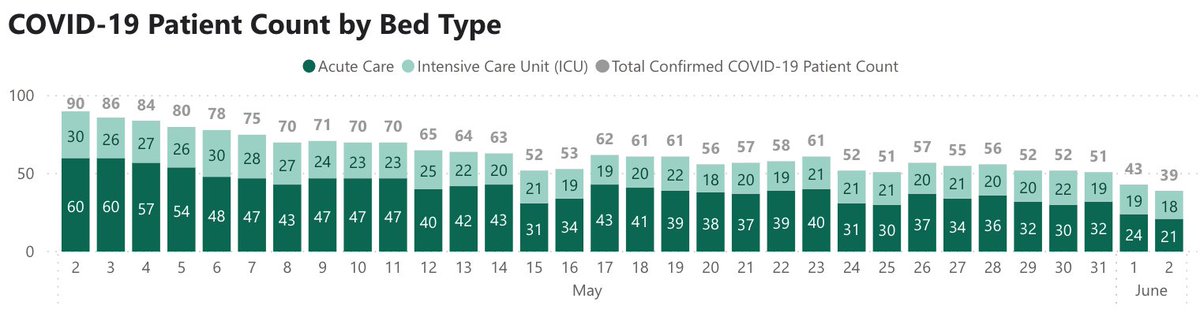
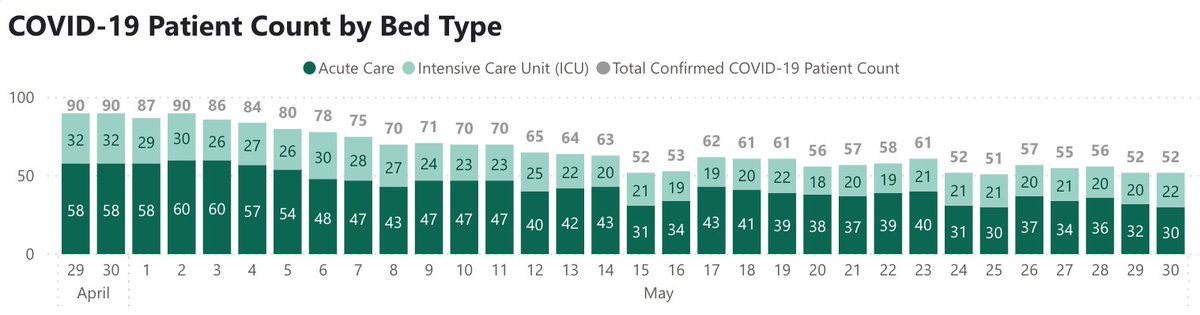
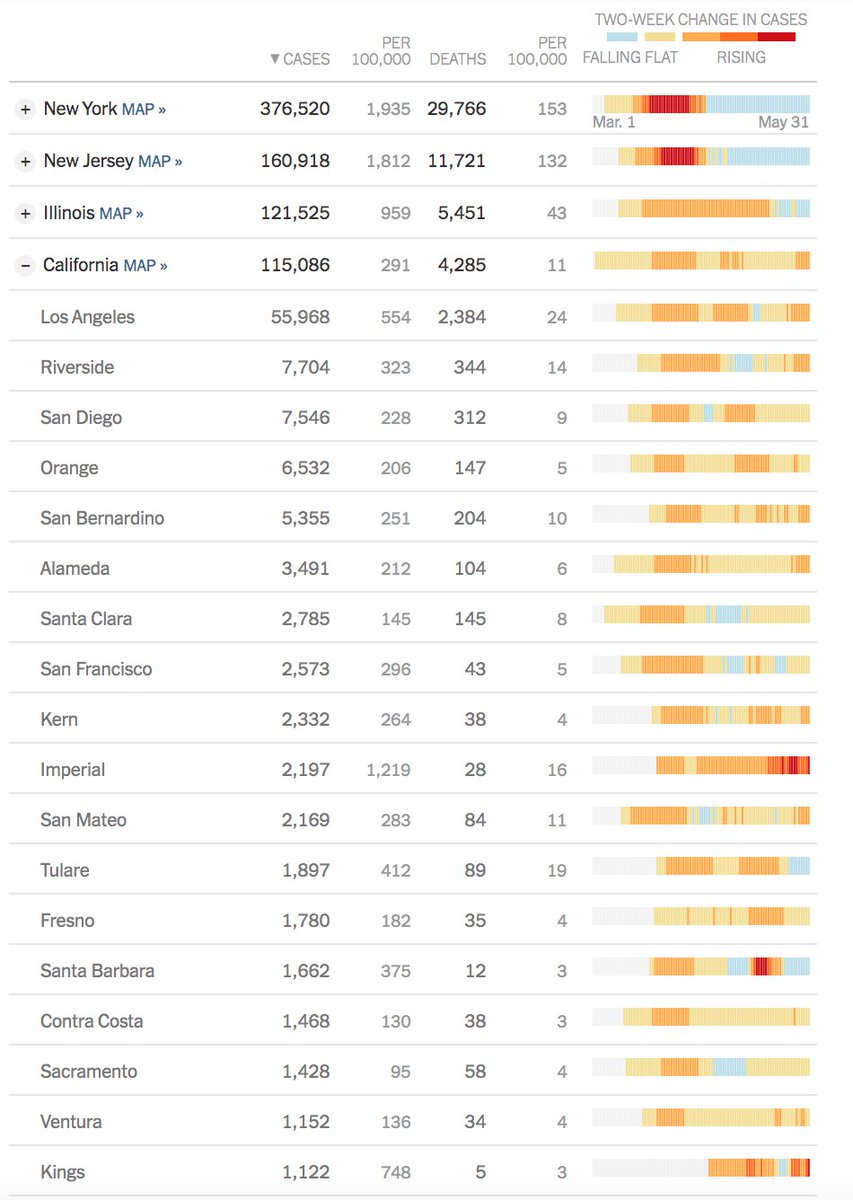
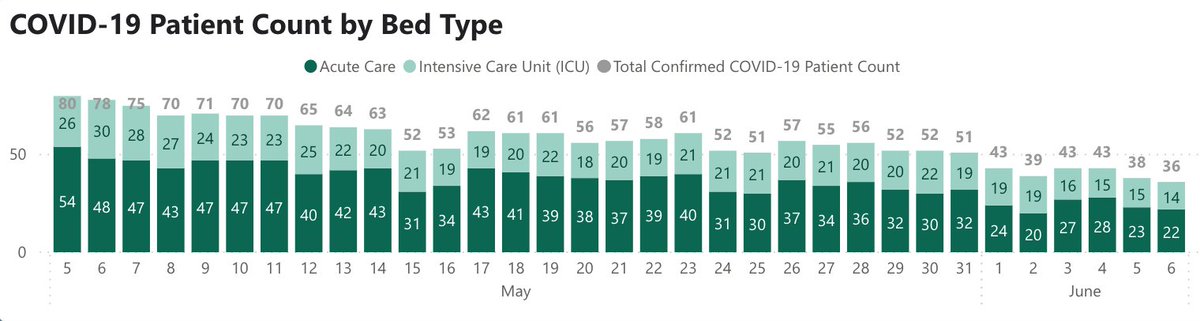
SF: new cases still ~25/d, but 0 deaths in 10 days. Hospitalizations down: 36, w/ 14 on vents – both #'s also lowest since March (Fig). CA surge all in southern CA
@ucsfhospitals, 10 pts, 2 on vents: fewest vented pts we’ve had since March.
SF: new cases still ~25/d, but 0 deaths in 10 days. Hospitalizations down: 36, w/ 14 on vents – both #'s also lowest since March (Fig). CA surge all in southern CA
2/ Still gathering more info re: @WHO announcement that asymptomatic transmission is “very rare” cnb.cx/3fa9xjb May well be LOWER risk than from pts w/ symptoms, but "very rare" violates all I know from research. I’ll lay odds that WHO walks this one back in a few days.
3/ Today, a riff on hospitals in the Covid era:
Hospitals care for the very sick, sometimes perform miracles, are where most Americans die, and are where we spend ~30% of our healthcare $'s. Hospitals were vital in Covid, but pandemic has dealt a huge blow to their bottom lines
Hospitals care for the very sick, sometimes perform miracles, are where most Americans die, and are where we spend ~30% of our healthcare $'s. Hospitals were vital in Covid, but pandemic has dealt a huge blow to their bottom lines
4/ Hospitals have long been felt to be “recession-proof,” but we now know that’s not true. Hospitals are like airplanes: with huge fixed costs, they need to run full. (Until/unless the payment system changes from mostly fee-for-service to capitated or “value-based” payments.)
5/ As with other businesses, Covid led us to shut down as much as we could. But unlike "normal" businesses, hospitals needed to stay very much open, both for Covid patients and for other emergencies. So we cut all non-urgent work, including surgeries, procedures, & clinic visits.
6/ Nor could we lay off staff – we needed all hands on deck in case of a Covid surge. So we saw very little savings on our usual costs & had many new costs (PPE, testing, staffing), coupled w/ a huge reduction in income. During March/April, @UCSFHospitals we lost ~$5 million/day.
7/ In NYC, Boston, & other hot spots, hospitals were packed w/ Covid pts. In SF, we were fortunate not to be, so we sat half empty. Economics in both cases are equally dire. @UCSF, we’re projecting ~$700M in losses. @nyphospital, they’re in similar straits bit.ly/3dPJcqc
8/ Why? As Ian Morrison said in grand rounds bit.ly/3dRJblO, economics of hospitals driven by procedures in pts w/ commercial (mostly employer-based) insurance. Margins there allow us to lose money on pts with no insurance, or w/ Medicare/Medicaid. A fragile shell game.
9/ Of course, this economic model is dysfunctional – why should a hospital make its money off procedures? Why disincentivize primary care? Why don’t we pay based on “value” (outcomes divided by costs)? Why should employers subsidize the care of patients w/ government insurance?
10/ All true, but God help any politician who tries to change this system. Even Obamacare was mostly about getting people health insurance, steering far away from taking on financing, paying for value (vs. volume), & overuse. And passing it wasn’t a picnic, as you may recall.
11/ So every hospital in the U.S. (including @UCSF) is now trying to convince patients to come in for their visits, procedures, and surgeries. It’s mostly because the patients need the care, but it’s also because our economic survival depends on it.
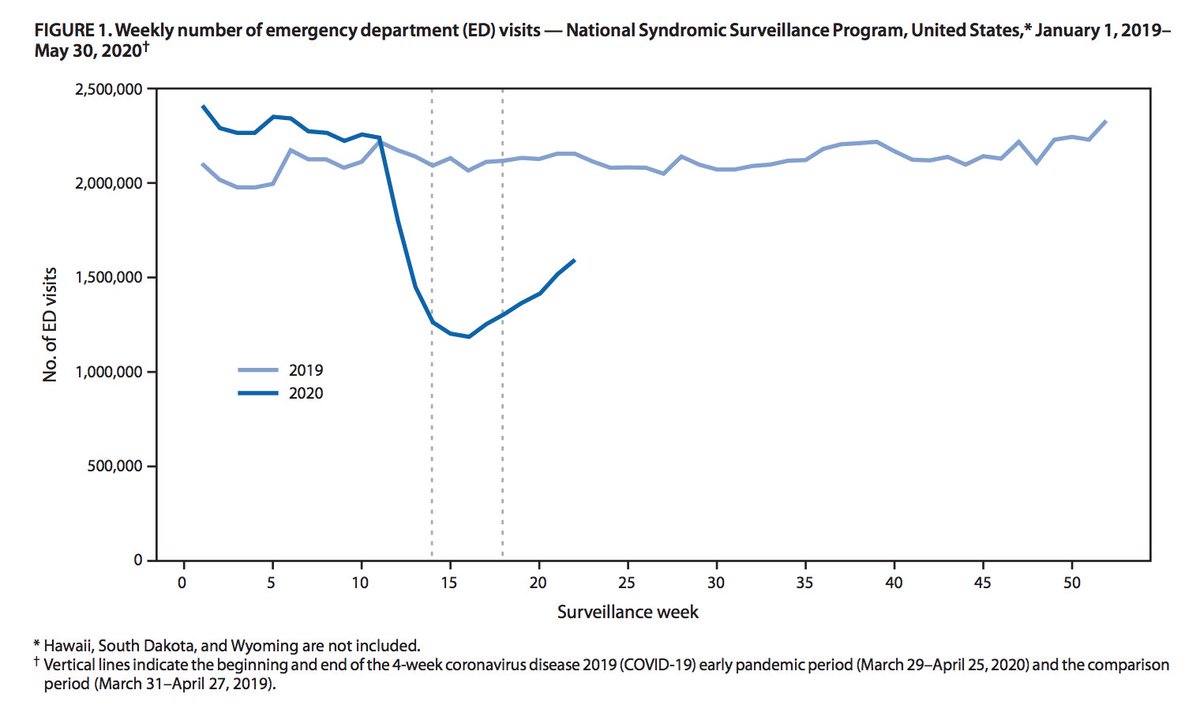
12/ In March, we purposely stopped everything but emergency surgeries, procedures, & outpatient visits. What shocked us was the number of emergency pts that stayed away (“where did all the heart attacks go?”). New @CDCgov data (Fig): 42% drop in ER visits bit.ly/2MHVaXa
13/ Some pts stayed away because of visitor restrictions nyti.ms/3ekQOky, now mostly eased. Now, pts staying away mostly due to fear of catching Covid. (Some also due to personal economic hardship.) Concern understandable, yet I feel safer in hospital than supermarket.
14/ At UCSF, volumes are now about halfway between our pre-Covid baseline (ie, packed) and where we were in March (ie, half-empty). Our financial losses are also ~half of what they were in March. So we’re doing better than we were 2 mths ago, but still crawling out of deep hole.
15/ Everybody worried re: hospitals being overrun by Covid, yet most managed to fit pts in 7ny.tv/30t19XX. Turns out hospitals are fairly flexible re: capacity: vented patients in recovery rooms, 2 pts on a vent, etc. Good to know for next pandemic (or next Covid surge).
16/ Economic crunch will likely cause some hospitals to fail. That’ll be a hit to a town, yet – unless it's v. isolated – new capabilities (particularly virtual care) may lower need for full-service hospital in every town. Of course, can’t deliver baby or do surgery via telemed.
17/ Today’s @nytimes on fed bailout ($175B) to hospitals nyti.ms/2Up5tU0 Makes point that large hospital systems received 100's of millions of dollars, mostly didn’t cut leadership comp (some >$10M/yr), and many laid off or furloughed staff despite taking federal money.
18/ @UCSFHospitals, FYI, we’ve received about $100M from feds, about 15% of losses. No layoffs, but they're not off the table if we don’t recover quickly. All MD/staff salaries frozen. Much depends on how next few months go – belt tightening everywhere but we may need to do more.
19/ A few other thoughts on hospitals in Covid era:
Re: telemedicine – we learned that not only can many (perhaps most) outpt visits go virtual, but also many hospital visits. This helped us lower # of visits (w/ lower PPE use & infection risk) & has big future implications.
Re: telemedicine – we learned that not only can many (perhaps most) outpt visits go virtual, but also many hospital visits. This helped us lower # of visits (w/ lower PPE use & infection risk) & has big future implications.
20/ For example, it would be great for @UCSF specialists to see a complex patient in another hospital’s ICU if hospital lacked needed specialty care. The devil will be in the details, but expect growth in telemedicine to have large impact on hospital, not just outpatient, care.
21/ With ↑telemedicine, another question: will “Hospital-at-Home” finally hit tipping point? Lots of data that, for select pts, HaH leads to equal outcomes at far lower costs than hospitalization bit.ly/2UpPDIW Yet its adoption curve has been glacial. Is its time now?
22/ Telemedicine solves one big problem: MD can now see patients daily & as needed. We’ve also gotten better w/ equipment (home IVs, O2) & tech (sensors). Yet still haven’t hit tipping point for HaH, despite 20 yrs of data. Need 2 things: payment system alignment & ease-of-setup.
23/ For an ED doc seeing a sick patient – if a hospital admission requires one phone call, whereas organizing HaH takes ten (bed, IV, O2, monitors, home nursing…), it’s just not gonna happen. Has to be one-stop-shopping, along w/ financial incentives that don’t stand in the way.
24/ In talking hospital finances, it's crucial that we not forget pts… and clinicians. @washingtonpost piece on brutal experiences of MDs, RNs, EMTs in hardest-hit Covid areas wapo.st/2Urx3QK. Too much death, fear, & impossible moral choices. Now PTSD in many. So sad.
25/ That’s it. It seems like volume of Covid news is slowing a bit. So this’ll be last Monday thread. I’ll still post threads on Thurs (Grand Rds) & Fri weekly recap. Plus others as events dictate. Goal is to update, but not oversaturate.
Back Thurs for grand rounds. Stay safe.
Back Thurs for grand rounds. Stay safe.