
Stunning fact: Not even one single developed country has >1000 COVID cases per day. We have >50,000 per day in the United States.
Epic failure of leadership at National level, as well as at the State level in many states. @ASlavitt @choo_ek @MelissaJPeltier @jeremyphoward
Epic failure of leadership at National level, as well as at the State level in many states. @ASlavitt @choo_ek @MelissaJPeltier @jeremyphoward

Normalizing to million population underestimates the severity of the epidemic in large countries. Ultimately it’s about the numerator: >50,000 new persons with COVID every day
Except Sweden, which made the wrong decision not to lockdown, there are no developed countries near us.
Except Sweden, which made the wrong decision not to lockdown, there are no developed countries near us.
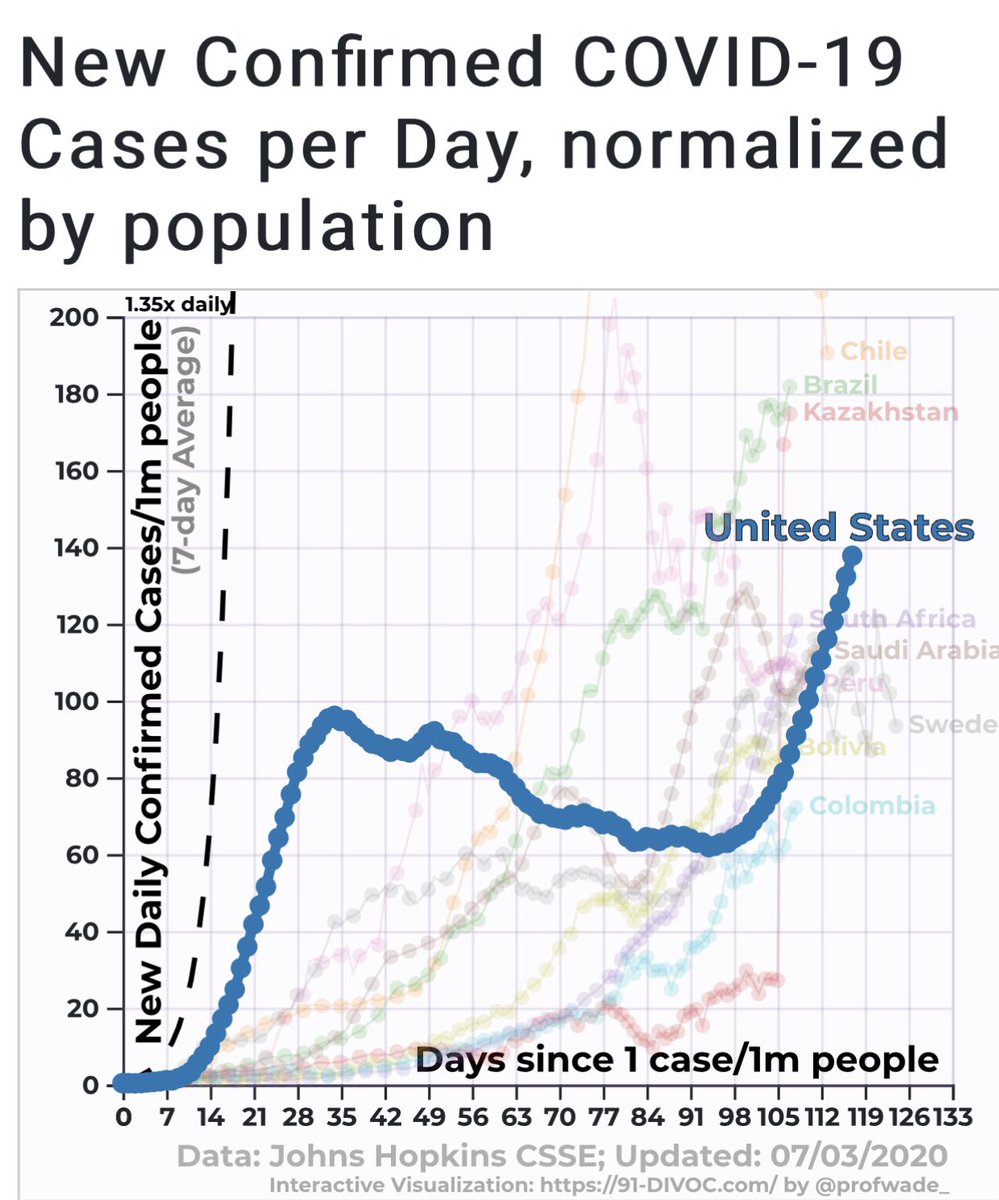
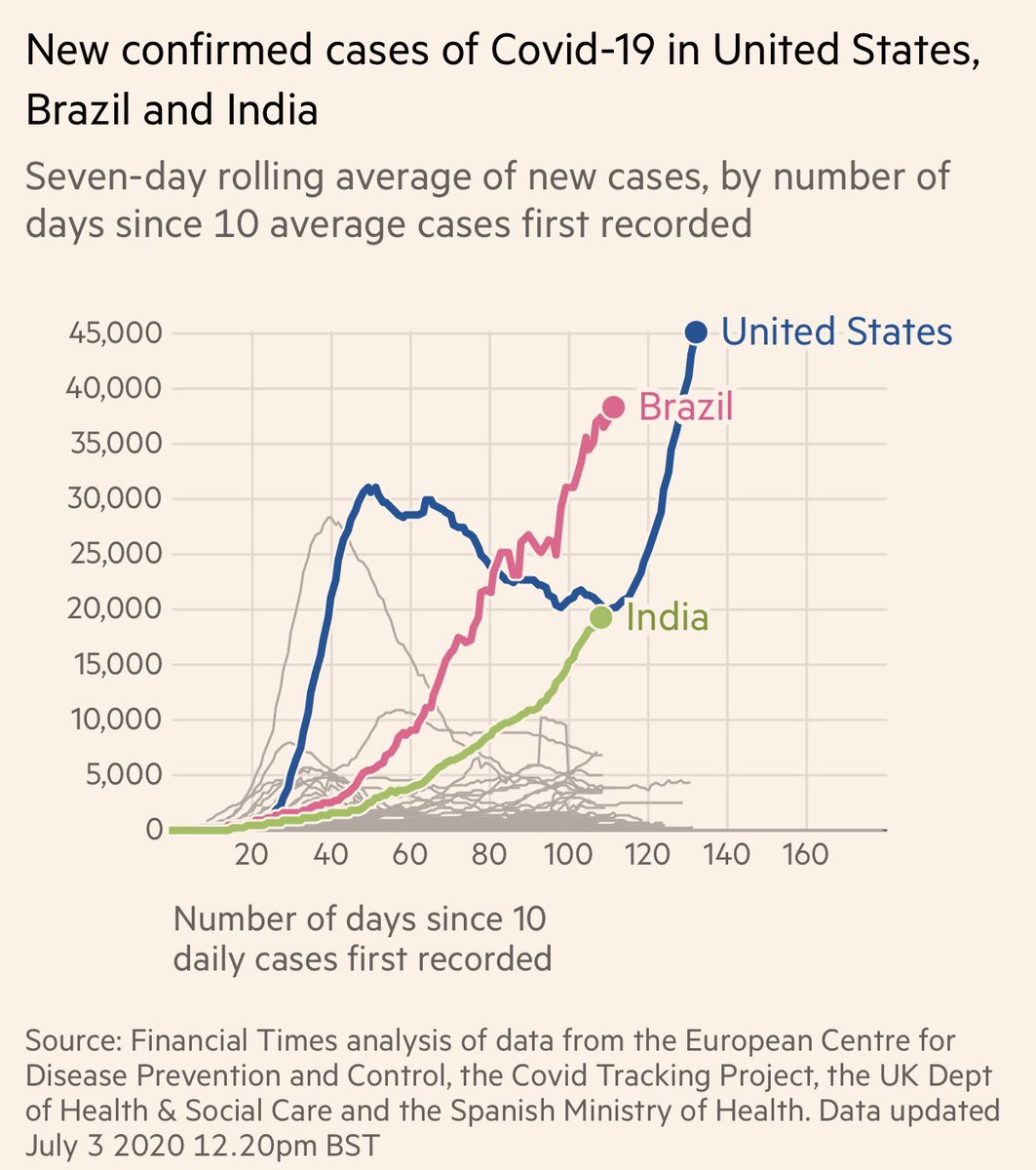
In case people are wondering who are our neighbors in the first tweet. Brazil overtook is for a short while. But we blew past them.
I’ll say the #1 reason for our failure is that FL, AZ, GA, CA, and TX did not mandate #Masks4All. @jeremyphoward
CA, TX do so now. But late.
I’ll say the #1 reason for our failure is that FL, AZ, GA, CA, and TX did not mandate #Masks4All. @jeremyphoward
CA, TX do so now. But late.
Overall doesn’t look very good.
https://twitter.com/joshtpm/status/1279177246738087936
One way of looking at COVID is to examine the US as multiple different countries and make appropriate adjustments for prevention, analysis, and mitigation strategies. It provides hope. Also supports plans by NY, Chicago to restrict entry. @chicagosmayor @NYGovCuomo
https://twitter.com/VincentRK/status/1276159410264576000
• • •
Missing some Tweet in this thread? You can try to
force a refresh


















