
1-So as most of you know, we published in @NEJM this week. This was so important for us for many reasons but fist a recap/summary of the paper.nejm.org/doi/full/10.10…
2/In low resource settings, WHO recommends standard of care for management of common illnesses in non-school going children. These illnesses include diarrhoea, pneumonia, malnutrition ; among others. 

3/ Pneumonia is commonly called ARI ( acute respiratory illness) and classified into no, mild or severe pneumonia. For our study we decided to study mild pneumonia.
4/ The diagnosis of pneumonia is made clinically, though counting respiratory rate or looking for chest indrawing or other signs of systemic infection in a child with cough or difficul breathing
5/The respiratory rate is counted via a timer and cut points are used to define pneumonia. A rate of 50 per min or more for infant and 40 per min or more for child is considered pneumonia. If it occurs in absence of indrawing or dangerous signs of infection, it’s non-severe/mild
6/ For mild fast breathing pneumonia, a simple 3 day course of antibiotic is prescribed.

7/ This is in conflict with recommendations of @IDSA and @PIDSociety where withholding is recommended for young children with mild pneumonia
8/Not give antibiotic for pneumonia? 😳 Does it even make sense? Seems like it may. thelancet.com/journals/lance…
9/ The biggest study looking at causes of pneumonia in South Asia and Africa identified viruses as the major cause of pneumonia in young children. This was conducted in hospitalised children.
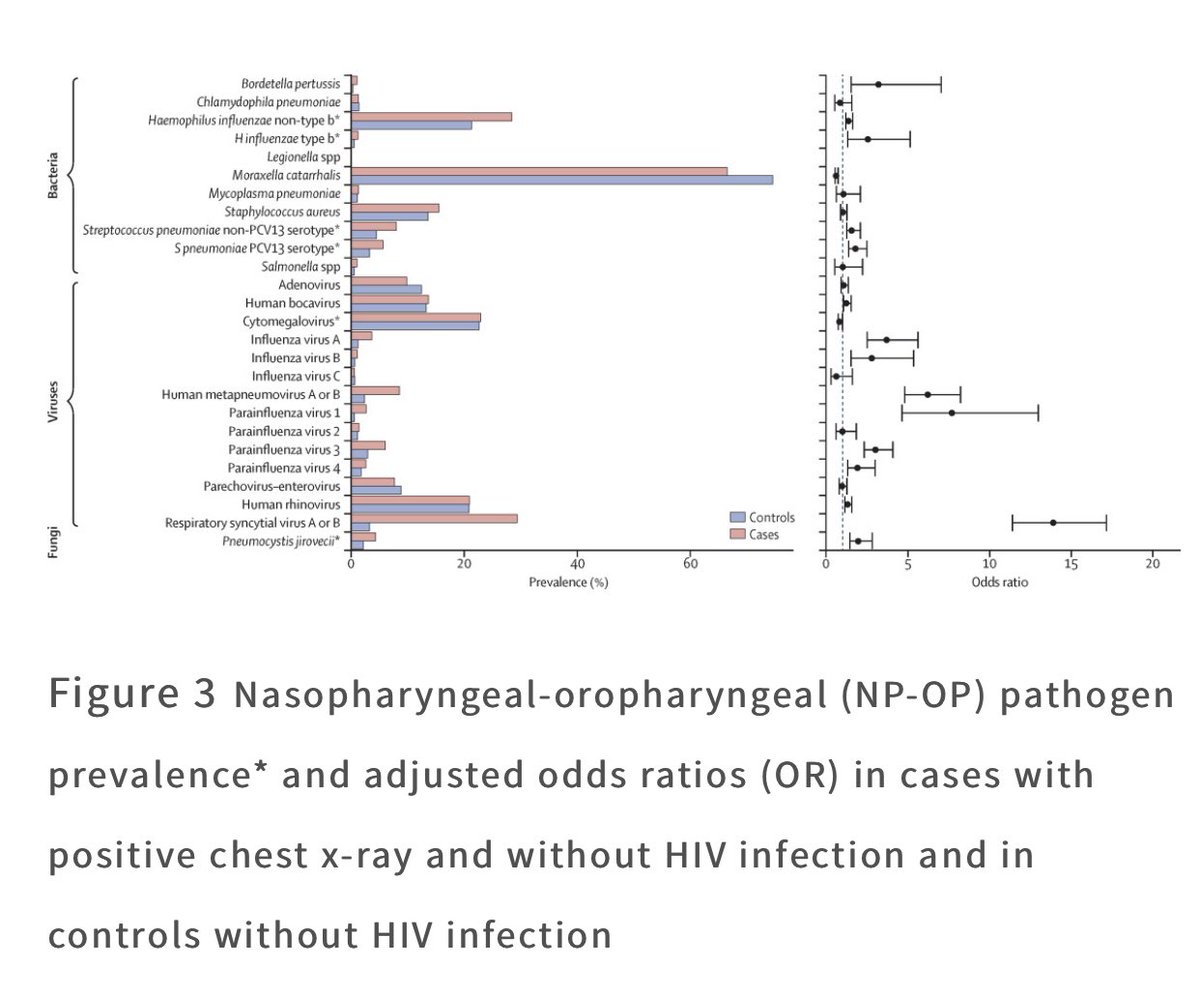
10/ But wait. There are bacteria 🦠 too. This bug called Streptococcus Pneumonia causes the highest deaths from pneumonia in children. Is counting respiratory rate enough?
11/ It may be, according to a review of evidence by WHO. But the strength of recommendation is moderately weak apps.who.int/iris/bitstream…
12/ This summary is getting rather long...please bear with me ...because I love you guys
13/ Even if the infection is viral, the children in these settings are malnourished, may have delay in seeking help and may be at risk of dying from bacterial pneumonia. The net thrown in to find these children has to be wide enough. Cannot let any child die from #pneumonia
13/ The WHO guidelines made sense with few caveats- 1. Strength of recommendation could be improved 2-Vaccines to prevent children from bacterial infections were being given 3- Amoxicyllin yet cheap and with a slow path to resistance, could still effect microbiome and growth
10-15 percent of children can have recurrent episodes with cumulative harm of anti tic use when not needed bmjopen.bmj.com/content/10/1/e…
14/ So we set to assess in an RCT, if withholding Abx is safe. The study was funded generously through @The_MRC @gatesfoundation and @DFID_UK and @wellcometrust
15/4002 children were randomised to get Abx (standard of care) or placebo( test treatment). The numbers are the following 👇🏻

16/ Interesting findings during study conduct were 1. Very few were failing treatment ( we didn’t know who at that point because we were blinded) 2. there were many children coming back with recurrent episodes making enrolment challenging. We adapted on the sample size (doubled!)
17/ There was extensive follow up-yes that affects trial implications in real world-but safety was a huge concern. So we were navigated by a group of very able and senior scientists and epidemiologists. They formed our DSMB (the safety board) and TSC (the advisory)

18/There were high rates of stunting and wasting in our study, much like our other non-study kids. Every 1 in 3 child had fever and less than 10% enrolled were wheezers - arms were balanced for these important explanatory factors

19/ I forgot to mention that this was a non-inferiority design- meaning we weren’t looking to see if placebo was better than antibiotic (as if!). We were assessing if it was not much worse!

20/ This study design is always hard to justify and hard to prove. Most experiments are looking for a better treatment that can be done with a much smaller sample size. Not this one-hence the large sample size. nejm.org/doi/full/10.10…
21/ We checked on the children everyday until 3 days to see if they were worse. At the end of the study, we analysed the data blinded by arm. The arms ( Abx or placebo) were revealed in an in person meeting with our TSCand DSMB
22/ We were surprised by the results because placebo was doing a little worse than Abx, very little - but enough to tip our scales

23/ But we had large number to conclude that 95% of the children were getting better without Abx! So even if they were getting worse, the number was small. How worse did they get? ...read on.
24/ Sadly 2 children died, only 0.01% , one in each arm....but it was in a selected sample inspite of all safety nets. In the absence of these safety nets, 5% could be higher or they could get much worse.
25/ Looking at it another way, we learnt that to prevent that one child from getting worse, we had to treat many many more -44 to be exact. We need to get better at finding that 1 child before we withhold Abx
26/ That ladies and gentlemen is work in progress- and I hope will make for a useful story one day. END OF THREAD Here’s our remarkable study team in a video

This thread got broken, can find another thread frm number 14 onwards

