💥How to use Urine Electrolytes for assesment & diagnosis of Kidney Disorders?
A great article in @CJASN
👉🏽 cjasn.asnjournals.org/content/14/2/3…
⚡️Summary of the article is in this🧵
#MedEd
#FOAMed
#NephPearls
A great article in @CJASN
👉🏽 cjasn.asnjournals.org/content/14/2/3…
⚡️Summary of the article is in this🧵
#MedEd
#FOAMed
#NephPearls
💥Urine Na is used for:
⚡️Assessment of effective circulatory volume
⚡️Differentiation of Pre-renal Azotemia vs. ATN
⚡️Assessment of effective circulatory volume
⚡️Differentiation of Pre-renal Azotemia vs. ATN
💥Spot Urine Na
⚡️Urine Na < 15 mEq/L suggests ⬇️ effective circulatory volume BUT the caveat is:
‼️Spot Urine Na is dependent on the amount of ‘water’ in the urine
⚡️Hence spot Urine Na can be ⬇️ in the setting of water diuresis & ❌ always mean ⬇️ volume
⚡️Urine Na < 15 mEq/L suggests ⬇️ effective circulatory volume BUT the caveat is:
‼️Spot Urine Na is dependent on the amount of ‘water’ in the urine
⚡️Hence spot Urine Na can be ⬇️ in the setting of water diuresis & ❌ always mean ⬇️ volume
💥This is why we use Fractional Excretion of Sodium: FeNa
FeNa = (UNa x PCr/ PNa x UCr) x 100
⚡️FeNa provides a measure of Urine Na handling independent of urine concentration (meaning independent of the ‘water’ in the urine)
FeNa = (UNa x PCr/ PNa x UCr) x 100
⚡️FeNa provides a measure of Urine Na handling independent of urine concentration (meaning independent of the ‘water’ in the urine)
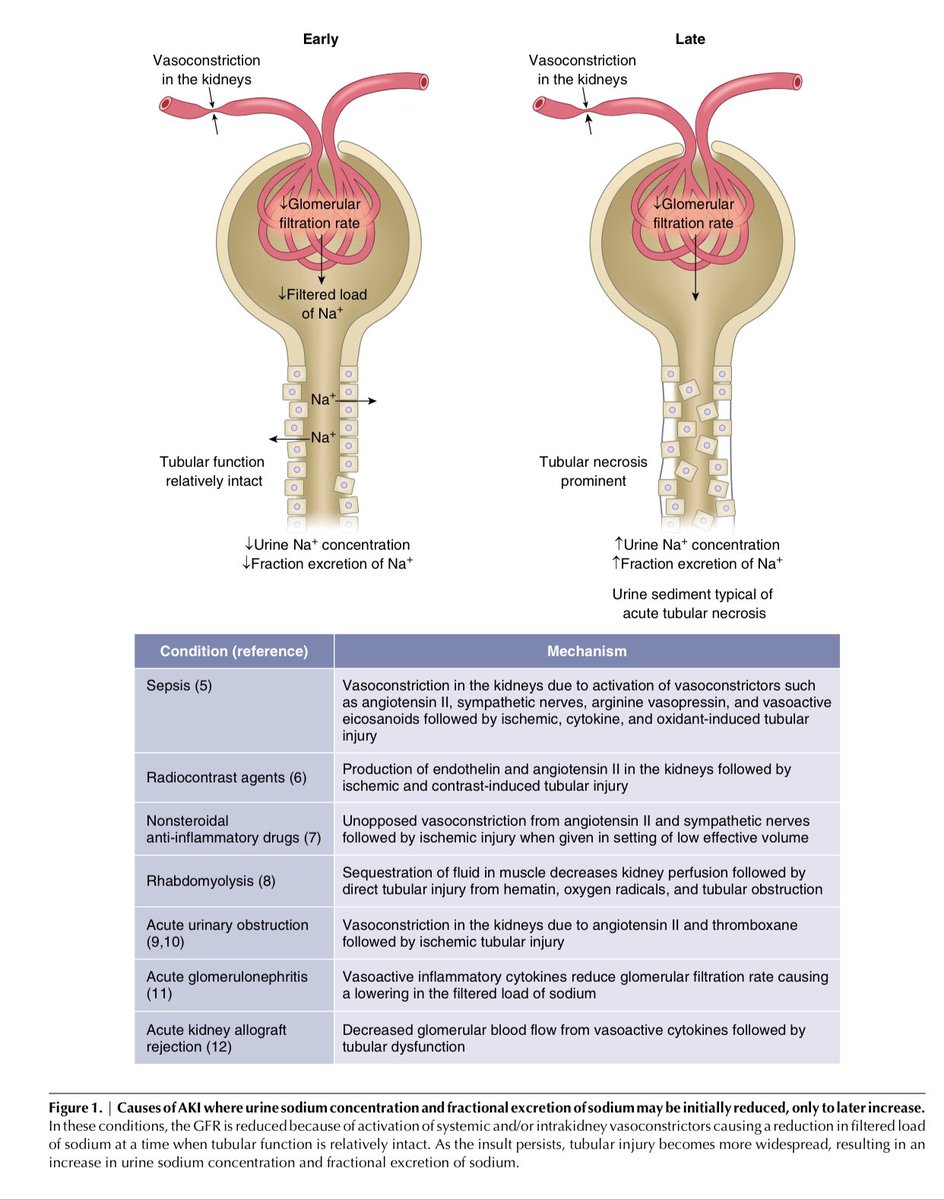
💥FeNa is used to differentiate b/w Pre-Renal Azotemia & ATN
⚡️FeNa < 1% suggests Pre-renal Azotemia & hence volume-responsive whereas a ⬆️ FeNa suggests ATN and hence not volume-responsive
‼️But FeNa is NOT always reliable in making this distinction
⚡️FeNa < 1% suggests Pre-renal Azotemia & hence volume-responsive whereas a ⬆️ FeNa suggests ATN and hence not volume-responsive
‼️But FeNa is NOT always reliable in making this distinction
💥Limitations of FeNa:
⚡️There are conditions that cause ATN but also cause intense renal vasoconstriction resulting in ⬇️ filtered load of Na, resulting in
⬇️ FeNa despite presence of ATN👇🏽
⚡️Sepsis
⚡️IV contrast
⚡️NSAIDs
⚡️Rhandomyolysis
⚡️There are conditions that cause ATN but also cause intense renal vasoconstriction resulting in ⬇️ filtered load of Na, resulting in
⬇️ FeNa despite presence of ATN👇🏽
⚡️Sepsis
⚡️IV contrast
⚡️NSAIDs
⚡️Rhandomyolysis
💥FeNa can also be misleadingly ⬇️ in the following conditions despite presence of ATN:
⚡️CHF
⚡️Cirrhosis
⚡️Extensive burns
‼️Intense neurohumoral activation =
Low FeNa
⚡️CHF
⚡️Cirrhosis
⚡️Extensive burns
‼️Intense neurohumoral activation =
Low FeNa
💥FeNa can be misleadingly ⬆️ despite ⬇️ effective circulatory volume in the setting of diuretic use (due to natriureis):
‼️In this situation, Fractional Excretion of Urea (FeUrea) can be used
‼️In this situation, Fractional Excretion of Urea (FeUrea) can be used
💥FeUrea
= (Ur Urea x Pcr/ P Urea x Ucr)x 100
= < 35% suggests ⬇️ volume
⬇️ volume -> ⬆️ prox. tubular water & urea reabsorption ⬇️ FeUrea
‼️So w/ distal diuretic use, loop or thiazides, but NOT w/ proximal diuretic use, FeUrea can be of help
= (Ur Urea x Pcr/ P Urea x Ucr)x 100
= < 35% suggests ⬇️ volume
⬇️ volume -> ⬆️ prox. tubular water & urea reabsorption ⬇️ FeUrea
‼️So w/ distal diuretic use, loop or thiazides, but NOT w/ proximal diuretic use, FeUrea can be of help
💥FeNa can be misleadingly ⬆️ despite ⬇️ volume when:
⚡️⬇️ volume is accompanied by ⬆️ in non-reabsorbable anions in urine, such as HCO3-, as HCO3- is excreted in urine paired w/ Na+
‼️Use Urine Cl and NOT FeNa to assess volume status in met. alkalosis
⚡️⬇️ volume is accompanied by ⬆️ in non-reabsorbable anions in urine, such as HCO3-, as HCO3- is excreted in urine paired w/ Na+
‼️Use Urine Cl and NOT FeNa to assess volume status in met. alkalosis
💥This is why in metabolic akalosis, Urine Cl is used as a marker to determine whether the metabolic alkalosis would be responsive to Cl-containing IVF or not:
⚡️⬇️ Urine Cl: responsive to IVF
⚡️⬆️ Urine Cl: not responsive to IVF
⚡️⬇️ Urine Cl: responsive to IVF
⚡️⬆️ Urine Cl: not responsive to IVF
💥Urine Chloride (Cl) excretion mirrors Urine Na excretion & hence both move in the same direction in response to changes in the effective circulatory volume
‼️Except when volume changes are accompanied by Acid-Base disorders
‼️Except when volume changes are accompanied by Acid-Base disorders
💥If Urine Na to Urine Cl ratio is >1.6 in the setting of ⬇️ volume then:
⚡️An accompanying anion is causing obligatory Na loss in the urine despite an appropriately ⬇️ Urine Cl in response to neurohumoral activation due to ⬇️ effective circulatory volume
⚡️An accompanying anion is causing obligatory Na loss in the urine despite an appropriately ⬇️ Urine Cl in response to neurohumoral activation due to ⬇️ effective circulatory volume
💥If UNa to Ur. Cl ratio is >1.6 in the setting of ⬇️ circulatory volume then:
‼️Check Urine pH: this will help identify the Non-reabsorbable Anion causing the obligatory Na loss
⚡️Ur. pH 7-8 = Bicarbonaturia
⚡️Ur. pH < 6 = Ketoanions or Drugs
👇🏽👇🏽👇🏽
‼️Check Urine pH: this will help identify the Non-reabsorbable Anion causing the obligatory Na loss
⚡️Ur. pH 7-8 = Bicarbonaturia
⚡️Ur. pH < 6 = Ketoanions or Drugs
👇🏽👇🏽👇🏽


💥If the Urine Na to Urine Cl ratio is
< 0.7 in the setting of ⬇️ effective circulatory volume then that suggests:
⚡️An accompanying cation in the urine causing obligatory Cl loss
⚡️Eg. ⬆️ ammonium excretion in urine as it is excreted as ammonium chloride
< 0.7 in the setting of ⬇️ effective circulatory volume then that suggests:
⚡️An accompanying cation in the urine causing obligatory Cl loss
⚡️Eg. ⬆️ ammonium excretion in urine as it is excreted as ammonium chloride
💥Urine Cl is helpful in work-up of:
⚡️Metabolic Alkalosis &
⚡️Metabolic Acidosis
👇🏽👇🏽👇🏽
⚡️Metabolic Alkalosis &
⚡️Metabolic Acidosis
👇🏽👇🏽👇🏽

💥Urine Potassium (K)
⚡️In Hypokalemia,
Step 1: ✅ determine if K loss is renal or extra-renal
⚡️Check Spot Urine K
< 5-15 mEq/L = extra-renal K loss
> 40 mEq/L = renal loss
‼️But Spot Urine K can be misleading as it can vary w/ urine concentration
⚡️In Hypokalemia,
Step 1: ✅ determine if K loss is renal or extra-renal
⚡️Check Spot Urine K
< 5-15 mEq/L = extra-renal K loss
> 40 mEq/L = renal loss
‼️But Spot Urine K can be misleading as it can vary w/ urine concentration
💥To overcome this limitation of Spot Urine K one can use the following:
‼️Urine K to Urine Creatine ratio
⚡️Ratio of < 13 mEq/g
OR
⚡️Ratio of < 2.5 mEq/mmol
Both indicate extra-renal K loss
‼️Urine K to Urine Creatine ratio
⚡️Ratio of < 13 mEq/g
OR
⚡️Ratio of < 2.5 mEq/mmol
Both indicate extra-renal K loss
💥Once it is determined that hypokalemia is due to renal or extra-renal loss based on the:
Urine K to Urine Cr ratio then the next steps are:
Step 2: ✅Check BP & assess effective circulatory volume👇🏽
Step 3: ✅Plasma HCO3👇🏽
Step 4: ✅Urine Chloride👇🏽
Urine K to Urine Cr ratio then the next steps are:
Step 2: ✅Check BP & assess effective circulatory volume👇🏽
Step 3: ✅Plasma HCO3👇🏽
Step 4: ✅Urine Chloride👇🏽

💥Urine Anion Gap & Urine Osmolar Gap in Metabolic Acidosis
⚡️In normal anion gap matabolic acidosis, determine if the source of the acidosis is renal or extra-renal
⚡️Calculate Urine Anion Gap (UAG):
(Urine Na + Urine K) - Urine Cl
⚡️In normal anion gap matabolic acidosis, determine if the source of the acidosis is renal or extra-renal
⚡️Calculate Urine Anion Gap (UAG):
(Urine Na + Urine K) - Urine Cl
💥Positive UAG = source of met. acidosis is renal
💥Negative UAG = source of met. acidosis is extra-renal
‼️Why?
Because ⬇️ urine ammonium excretion by the kidney in the setting of metabolic acidosis means that the kidney is NOT getting rid of the acid
💥Negative UAG = source of met. acidosis is extra-renal
‼️Why?
Because ⬇️ urine ammonium excretion by the kidney in the setting of metabolic acidosis means that the kidney is NOT getting rid of the acid
💥Why is Urine Anion Gap positive in the setting of ⬇️ urine ammonium excretion?
Because ammonium is excreted as ammonium chloride, now recall the UAG equation:
(Urine Na + Urine K) - Urine Cl
So ⬇️ ammonium excretion in urine = ⬇️ Urine Cl = Positive UAG
Because ammonium is excreted as ammonium chloride, now recall the UAG equation:
(Urine Na + Urine K) - Urine Cl
So ⬇️ ammonium excretion in urine = ⬇️ Urine Cl = Positive UAG
💥Urine Anion Gap can also be misleading - Why?
⚡️Recall that in the UAG equation we are only accounting for Urine Na, K & Cl
‼️So presence of ANY unmeasured ions (besides Na, K, Cl) can be misleading:
⚡️Ketoacids
⚡️Na Hippurate
⚡️D-lactate
⚡️Recall that in the UAG equation we are only accounting for Urine Na, K & Cl
‼️So presence of ANY unmeasured ions (besides Na, K, Cl) can be misleading:
⚡️Ketoacids
⚡️Na Hippurate
⚡️D-lactate
💥When UAG is not reliable to assess urine ammonium excretion then use:
Ur. Osmolal Gap
Ur. Osm. Gap >100 mOsm/kg=⬆️ ammonium excretion= Met. acidosis cause is extra-renal
Limitations: Ur. Osm. Gap can be ⬆️ due to non-ammonium solutes (mannitol, alcohols)
Ur. Osmolal Gap
Ur. Osm. Gap >100 mOsm/kg=⬆️ ammonium excretion= Met. acidosis cause is extra-renal
Limitations: Ur. Osm. Gap can be ⬆️ due to non-ammonium solutes (mannitol, alcohols)

💥This🧵is a review of how to use the following urine chemistries to assess & diagnose kidney disorders
⚡️Urine Sodium
⚡️Fractional excretion of Na
⚡️Fractional excretion of Urea
⚡️Urine Chloride
⚡️Urine Potassium
⚡️Urine Anion Gap
⚡️Urine Osmolar Gap
End/
⚡️Urine Sodium
⚡️Fractional excretion of Na
⚡️Fractional excretion of Urea
⚡️Urine Chloride
⚡️Urine Potassium
⚡️Urine Anion Gap
⚡️Urine Osmolar Gap
End/