
1/ @STARRTAKI now published in @NEJM nejm.org/doi/full/10.10… – an updated thread follows below
#starrtaki #aki #FOAMcc @nephjc
@DrRonWald @CCCTG_ @anzicsctg @UKCCRGroup @ICCCTN @CIHR_IRSC @NIHRresearch @nhmrc @HRCNewZealand 🇨🇦🇦🇺🇦🇹🇧🇪🇧🇷🇨🇳🇩🇪🇫🇮🇫🇷🇮🇪🇮🇹🇳🇿🇨🇭🇺🇸🇬🇧
#starrtaki #aki #FOAMcc @nephjc
@DrRonWald @CCCTG_ @anzicsctg @UKCCRGroup @ICCCTN @CIHR_IRSC @NIHRresearch @nhmrc @HRCNewZealand 🇨🇦🇦🇺🇦🇹🇧🇪🇧🇷🇨🇳🇩🇪🇫🇮🇫🇷🇮🇪🇮🇹🇳🇿🇨🇭🇺🇸🇬🇧
2/ Current CPGs do not make strong recommendations (Not Graded) on when to start RRT in ICU patients with AKI, in the absence of urgent indications, due largely to discrepant findings from prior RCTs (bit.ly/3fKqEZy) (bit.ly/39etR0N) @goKDIGO @NICEComms
3/ The @STARRTAKI trial is the largest multinational trial (168 sites, 15 countries) to address whether an accelerated (early) strategy compared with standard (delayed) strategy impacts mortality and kidney recovery in ICU patients with AKI #generalizability
4/ The @STARRTAKI trial was unique from prior RCTs in that clinician equipoise was integrated into eligibility. This appropriately excluded 2196 patients who clinicians felt RRT should start immediately and 5690 patients who clinicians felt recovery was anticipated #equipoise
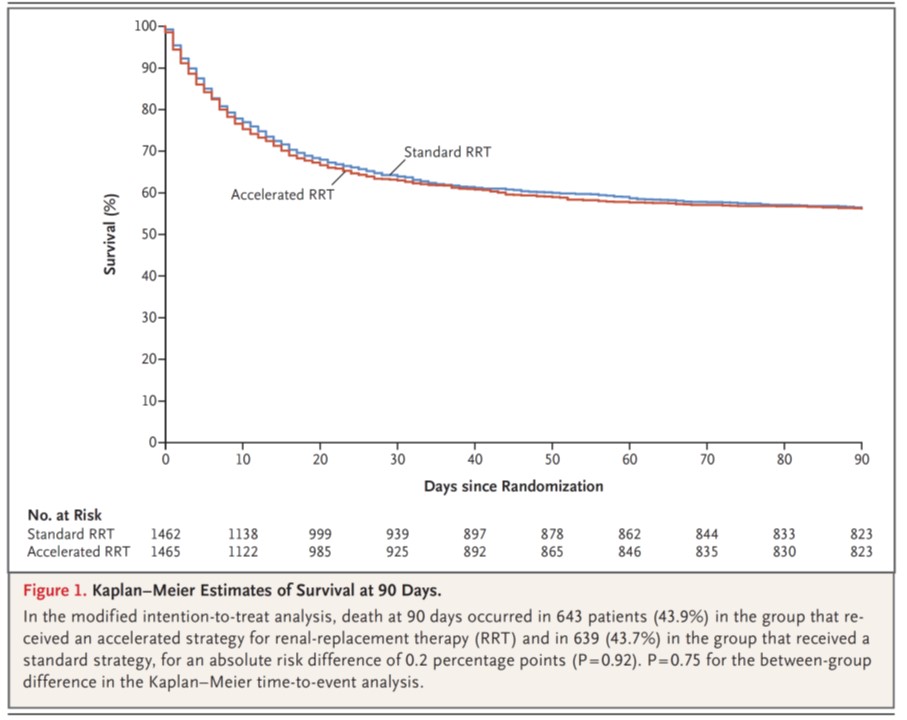
5/ @STARRTAKI - randomized 3019 patients (mITT cohort was 2927) to an accelerated-strategy for RRT (98.6% received RRT within 6.1 hr) or standard-strategy (61.8% received RRT within 31.1 hr)
6/ In @STARRTAKI - treatment arms were well balanced at the time of randomization: CKD in 43.8%; 67.0% medical; sepsis in 57.7%; 76.9% were mechanically ventilated; 70.4% receiving vasoactive therapy
7/ @STARRTAKI - for those starting RRT in the standard-strategy - only 66.1% had >= 1 trial-specific RRT indication - most commonly low P/F ratio with concern for volume overload (43.6%) and a time from randomization >= 72 hr (23.7%)
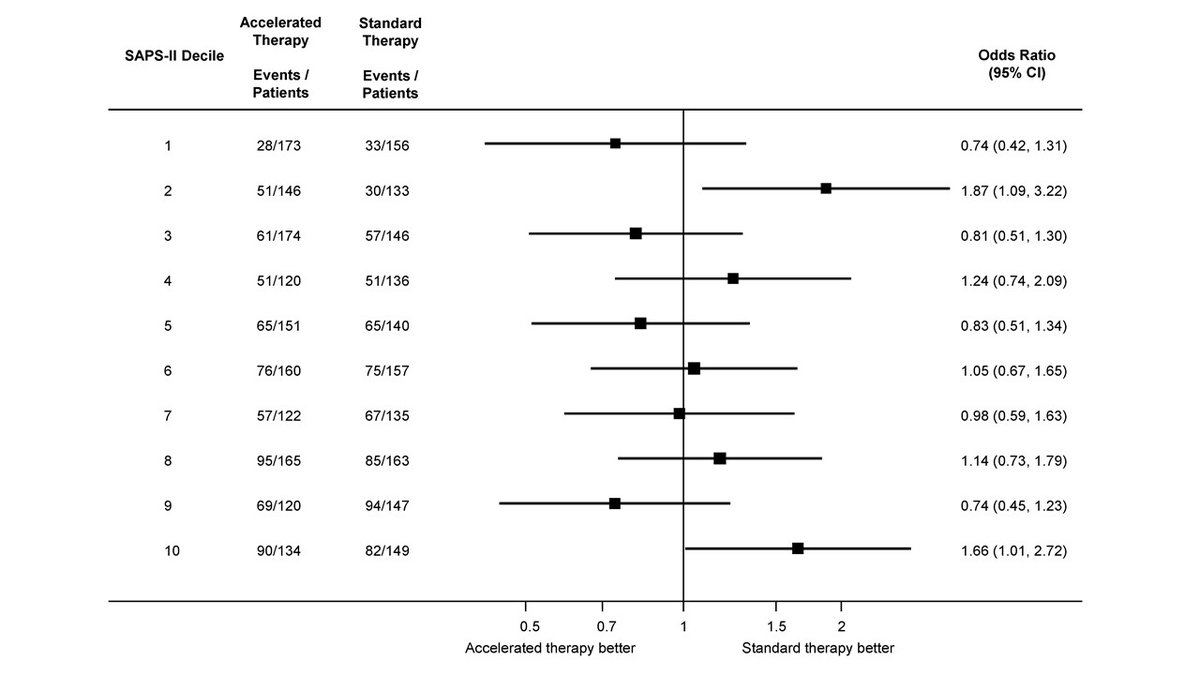
8/ @STARRTAKI - death at 90-days (primary): 43.9% in accelerated and 43.7% in standard (RR 1.00; 0.93-1.09). There was no heterogeneity in treatment effect across any pre-planned subgroups (sex, eGFR, sepsis, SAPS II, surgical, region) or by deciles of SAPS II score #robust 
9/ @STARRTAKI - RRT dependence at 90-days (secondary): 10.4% in accelerated and 6.0% in standard (RR 1.74; 1.24-2.43). This was #robust across several pre-planned sensitivity analysis
10/ @STARRTAKI - adverse events - largely focused on RRT complications - were more common in accelerated (23.0%) vs. standard (16.5%) - driven by more hypotension episodes and hypoPO4; no difference in serious AE
11/ @STARRTAKI - High-level thoughts on how these results may change practice:
No. 1: Given no evidence of survival difference; but risk of RRT dependence (NNH 23) and AE higher (NNH 16) and RRT use greater with an accelerated-strategy - watchful waiting would appear reasonable
No. 1: Given no evidence of survival difference; but risk of RRT dependence (NNH 23) and AE higher (NNH 16) and RRT use greater with an accelerated-strategy - watchful waiting would appear reasonable
12/ @STARRTAKI - No. 2: Reasons for greater RRT dependence at 90-days are not clear - but may relate to "dialysis-related" disruption of kidney repair/recovery - such as more iatrogenic hypotension; this is an important outcome for patients and health systems
13/ @STARRTAKI - No. 3: AE were greater in accelerated, but centered on RRT-related events and the accelerated had more days-at-risk; it is unclear if there was hazard to worsening AKI (or therapies to mitigate complications) in standard not receiving RRT
A summary slide below:
A summary slide below:
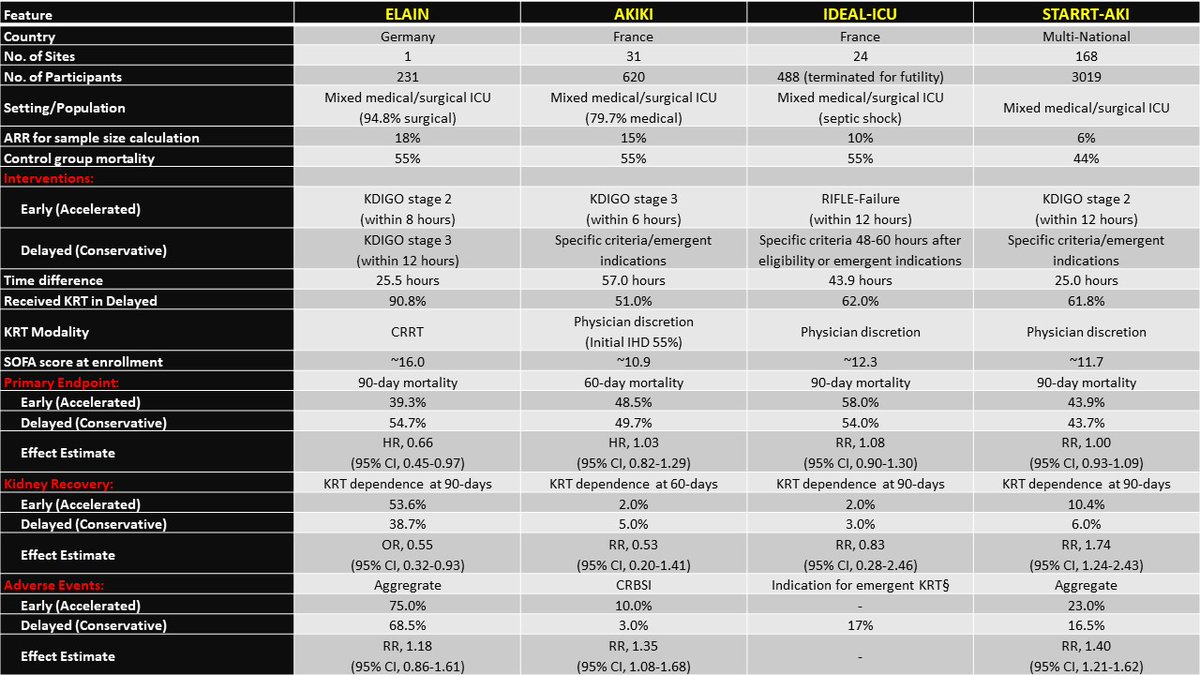
14/ Important implications for clinical practice; CPGs will need updating.
Big thx again to our huge team: @BellomoRinaldo @StephaneG05 @EricHoste @dfmcauley @ShayMcGuinness1 @Bram_Rochwerg
@DogICUma @orlasmith51 @javo_neyra @LiuKD @kidneybloke @AzraBihorac...
More to come...
Big thx again to our huge team: @BellomoRinaldo @StephaneG05 @EricHoste @dfmcauley @ShayMcGuinness1 @Bram_Rochwerg
@DogICUma @orlasmith51 @javo_neyra @LiuKD @kidneybloke @AzraBihorac...
More to come...

