
Cool paper from @DavidLBrownMD and Conor Williams in @Heart_BMJ exploring what would happen if we deferred PCI in diabetics with SIHD!
Mini-thread below
heart.bmj.com/cgi/content/fu…
Mini-thread below
heart.bmj.com/cgi/content/fu…
First, this is an example of data reuse from RCTs (in this case BARI-2D). Data are made available by @nih_nhlbi through BioLINCC repository. Some paperwork is required to ensure patient privacy, etc but process is usually straightforward & quick:
biolincc.nhlbi.nih.gov/studies/bari2d/
biolincc.nhlbi.nih.gov/studies/bari2d/
Another thing is this study reminded me that the outcomes of the PCI stratum in BARI-2D were actually numerically worse for the revasc arm vs. medical therapy:
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…

Using the endpoint of death or MI at 1 year, this was actually significantly worse for PCI than OMT alone.
One question from @DavidLBrownMD is how much of this was periprocedural? From KM plots looks like at least the MIs are likely to be, which some people dismiss as not all that important. However, in this case it is paralleled by a similar, but non-significant, excess of death.😱
The clever thing done by this team is something that is akin to a *randomization test*. What they did was randomly pretend that some of the PCI patients were deferred by substituting patients from the OMT arm in their place.
They did this lots of times with varying % of patients substituted. This is one form of Monte Carlo simulation, a generic term for a simulation where you repeatedly making a random change and seeing how it affects the outcome.
Obvs if everyone in the PCI arm was deferred, the outcomes would be essentially the same as in the OMT arm.
Conversely, if everyone in the PCI arm got treated the way they did in the trial, nothing much would change at all.
Conversely, if everyone in the PCI arm got treated the way they did in the trial, nothing much would change at all.
In between, you get a smooth reduction in adverse outcomes as you do less PCI.
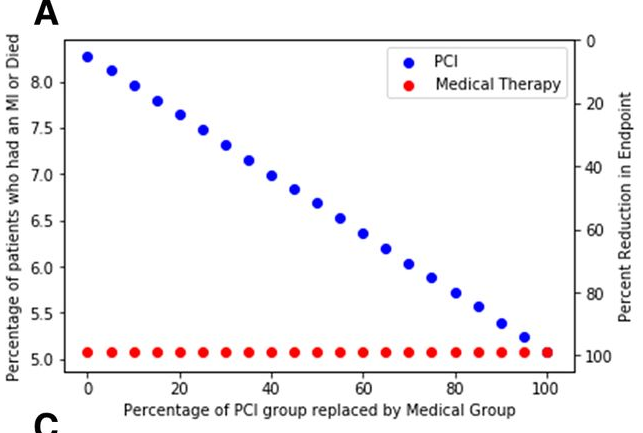
So, in some ways this isn't surprising. The moment you realize that PCI had worse outcomes, it kind of follows that less of it leads to better outcomes.
That said, this is a clever way to demonstrate that numerically and graphically.
That said, this is a clever way to demonstrate that numerically and graphically.
Some caveats - the revascularization outcome alone was neutral so this is a subgroup of an overall negative trial. That is partially mitigated because the randomization was stratified around this subgroup.
Also, over time the difference observed in the PCI stratum was non-significant it seems.
That said, it does seem there is a consistent message among many SIHD trials of early harm from PCI vs. OMT that may or may not reverse much later on. Similar results are seen in ISCHEMIA.
That said, it does seem there is a consistent message among many SIHD trials of early harm from PCI vs. OMT that may or may not reverse much later on. Similar results are seen in ISCHEMIA.
Overall, congratulations to @DavidLBrownMD and Conor Williams for a very clever analysis!
So, I misrepresented. This ended up being more than a MINI-thread.
But was this helpful?
But was this helpful?
• • •
Missing some Tweet in this thread? You can try to
force a refresh




