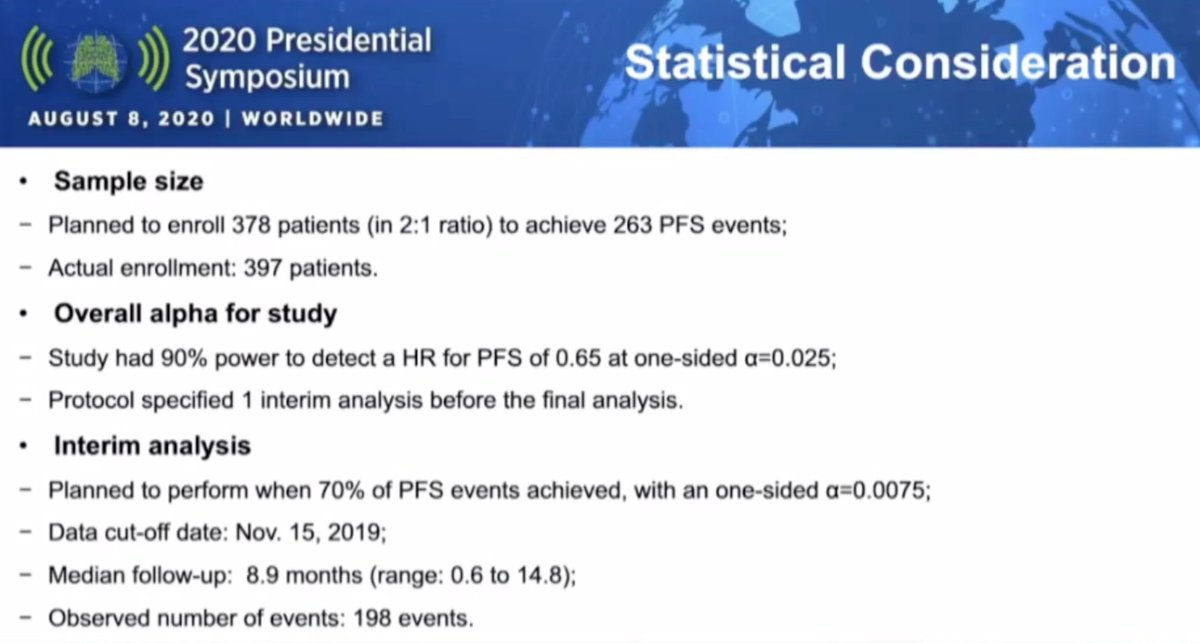
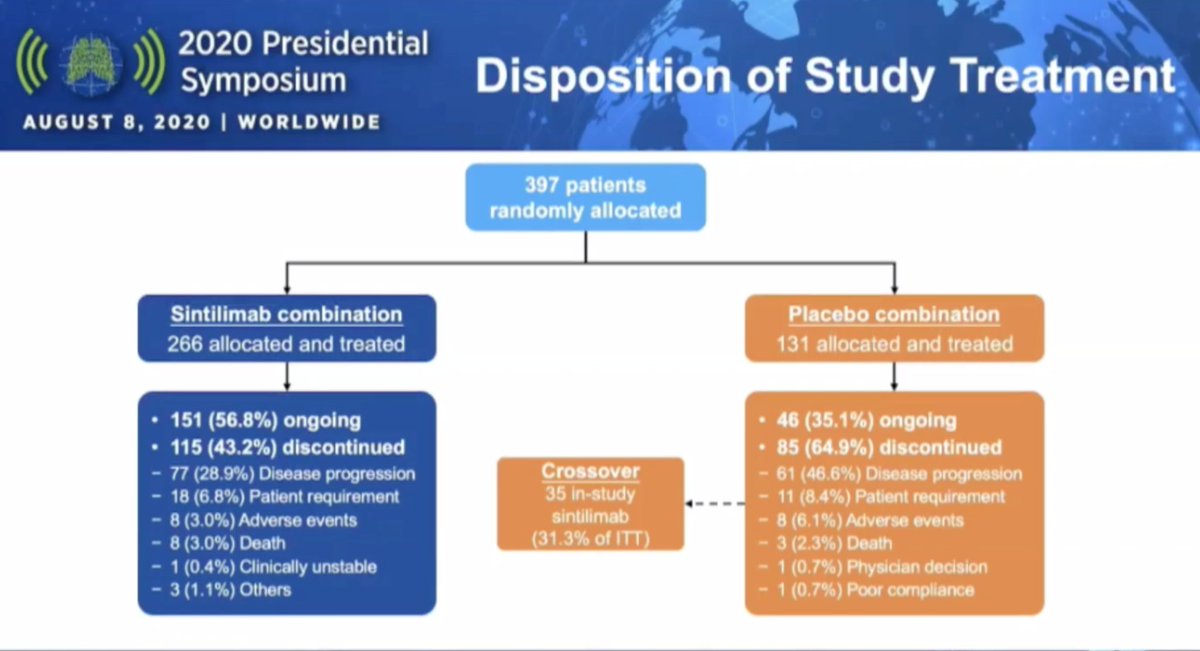
#VPS20 The ORIENT-11 trial presented by Dr. Zhang: 1L platinum/pemetrexed +/- sintilimab (anti-PD1) in non-sq NSCLC. Good design: 2:1 randomization, no EGFR/ALK, stratified by PDL1, crossover included. #LCSM @IASLC #WCLC20 
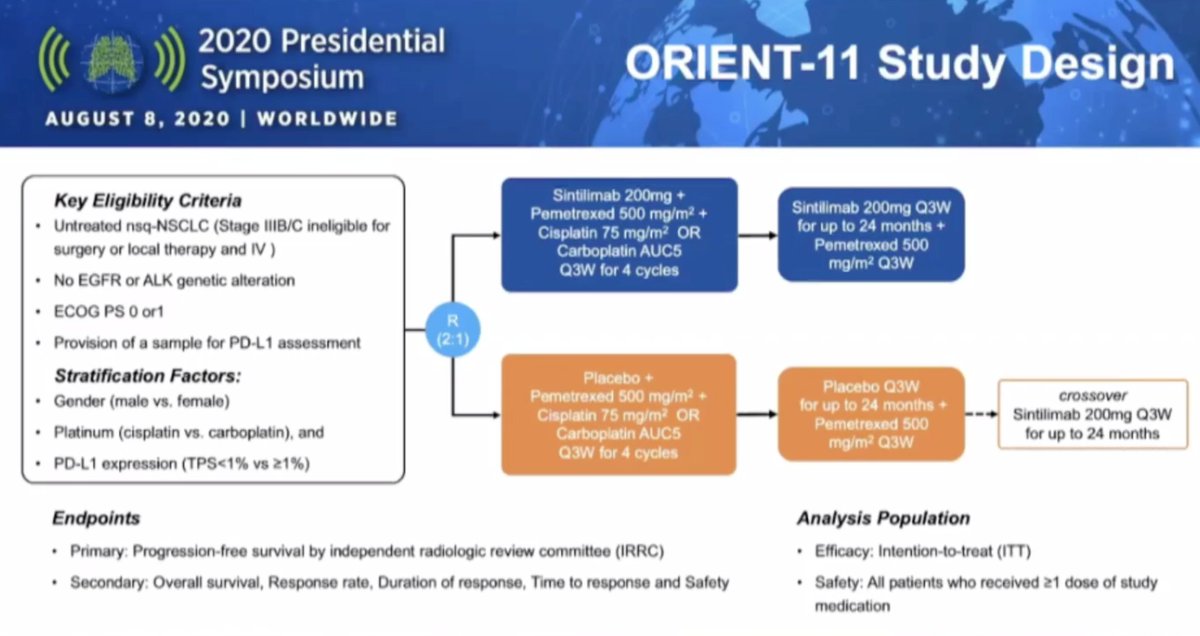
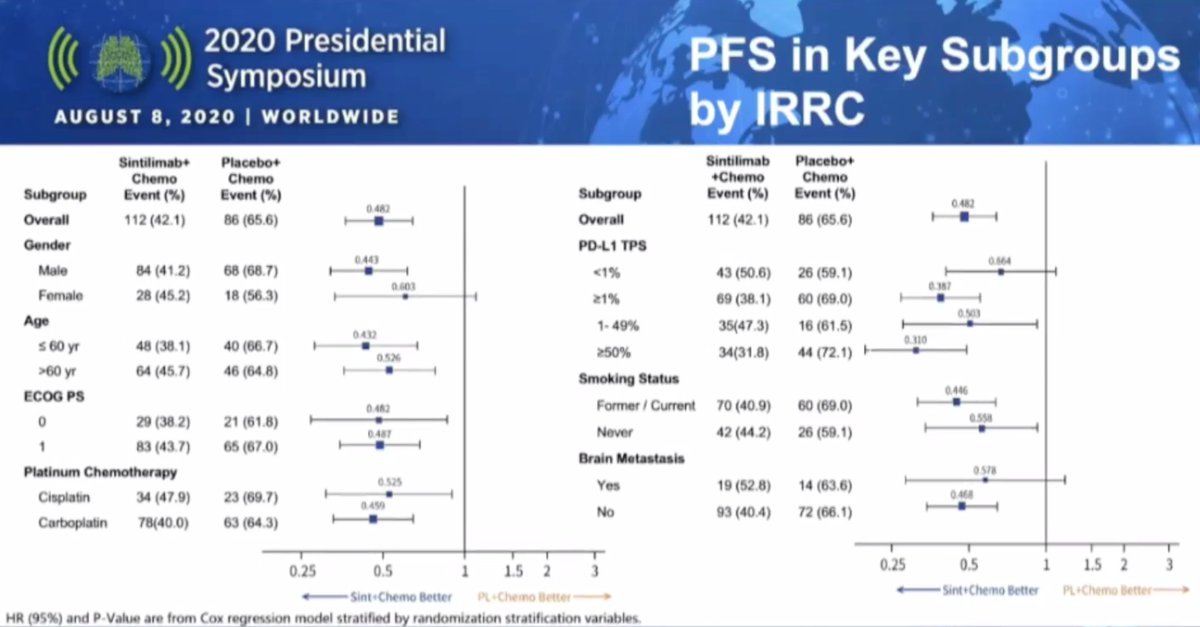
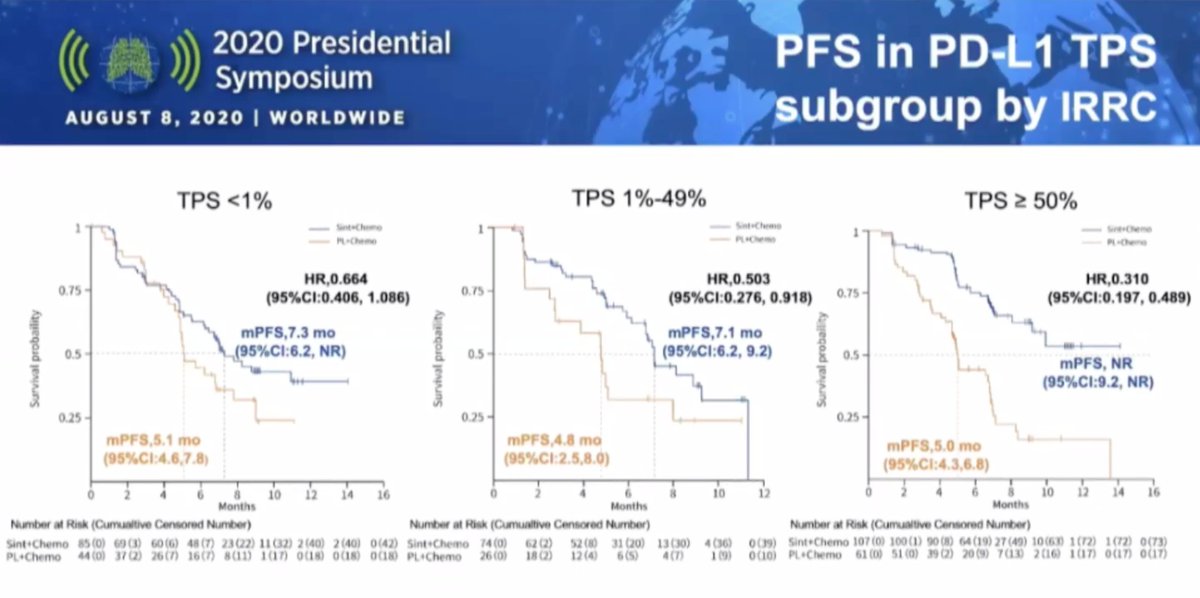
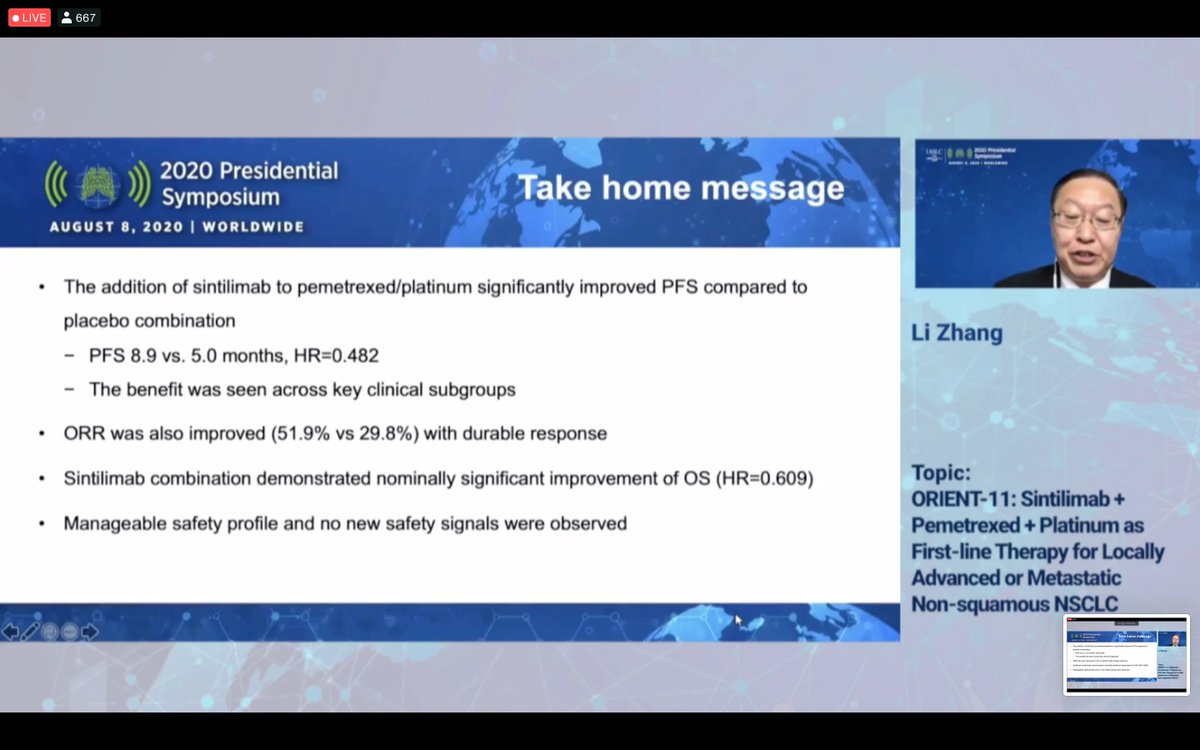
#VPS20 Positive study with PFS HR 0.482 favoring sintilimab, mPFS 8.9m vs 5.0m which is very comparable to KEYNOTE-189. Hits all the right subgroups and stepwise benefit by PDL1 expression. Important to have these data in an East Asian population. #LCMS @IASLC #WCLC20

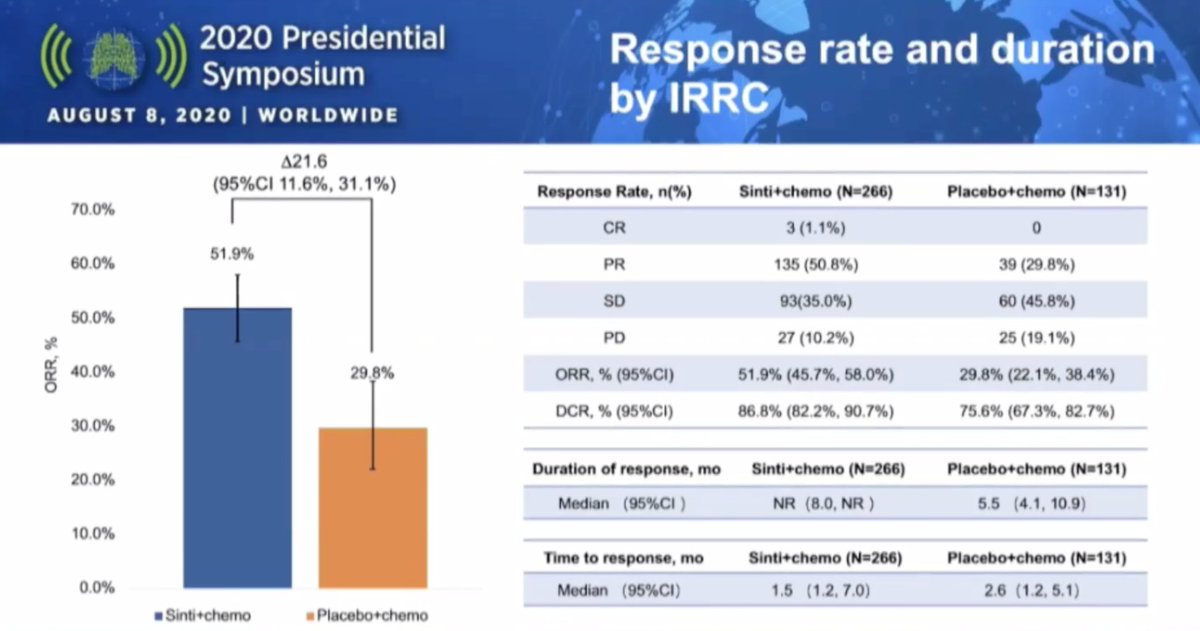
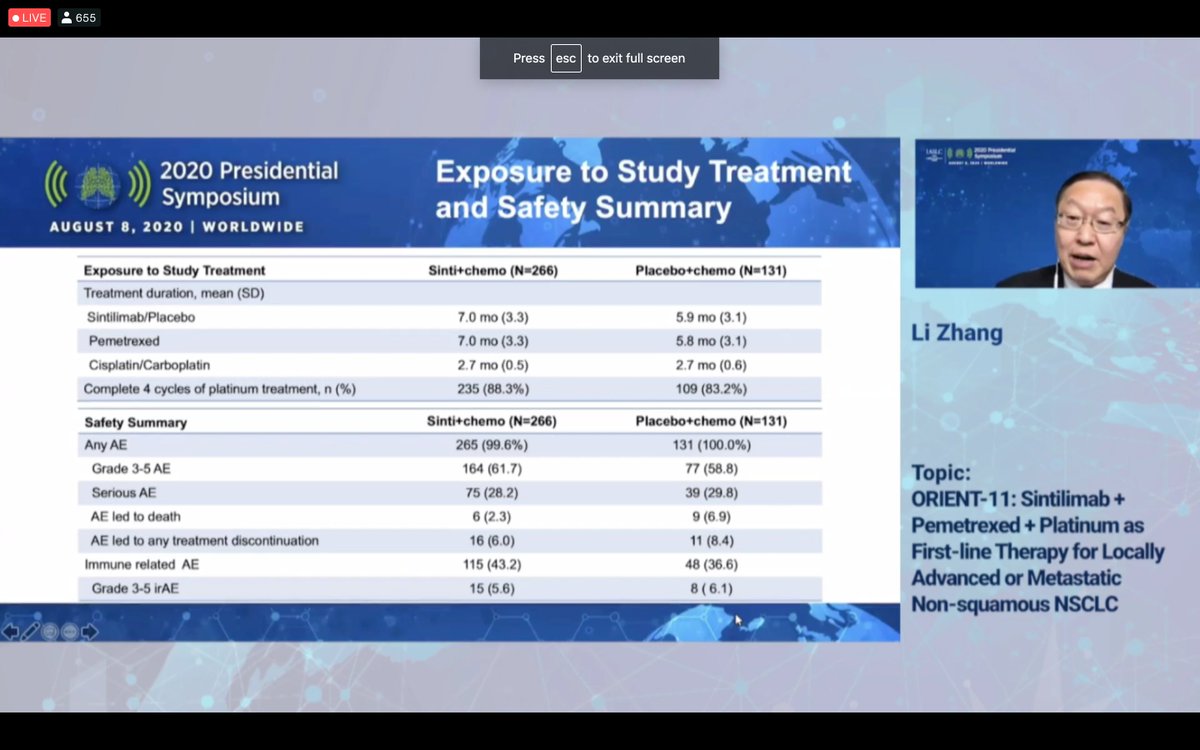
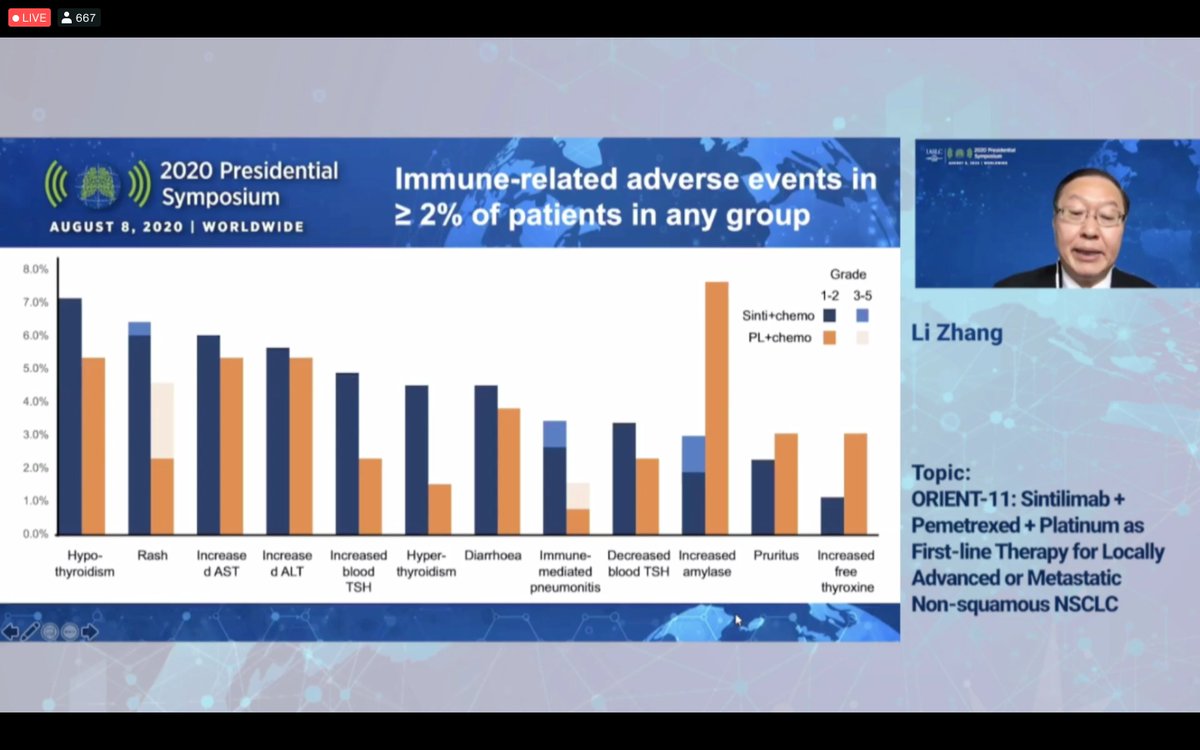
#VPS20 OS is immature but RR favors sintilimab (51.9% vs 29.8%), time to response 1.5 months and median duration not reached. No unexpected safety signals noted with this novel PD1 inhibitor in an East Asian population. #LCSM @IASLC #WCLC20

#VPS20 A crowded field but sintilimab compares favorably as a good option in East Asia and another active checkpoint inhibitor. #WCLC20 #LCSM @IASLC
• • •
Missing some Tweet in this thread? You can try to
force a refresh