1/ Covid (@UCSF) Chronicles, Day 149
Grand rounds today: . As we hit Covid’s 6 month mark in the U.S., we’re desperate for innovative approaches. Today, I decided to focus on 3 impressive ones – across a range of disciplines: testing, epi, & narrative.
Grand rounds today: . As we hit Covid’s 6 month mark in the U.S., we’re desperate for innovative approaches. Today, I decided to focus on 3 impressive ones – across a range of disciplines: testing, epi, & narrative.
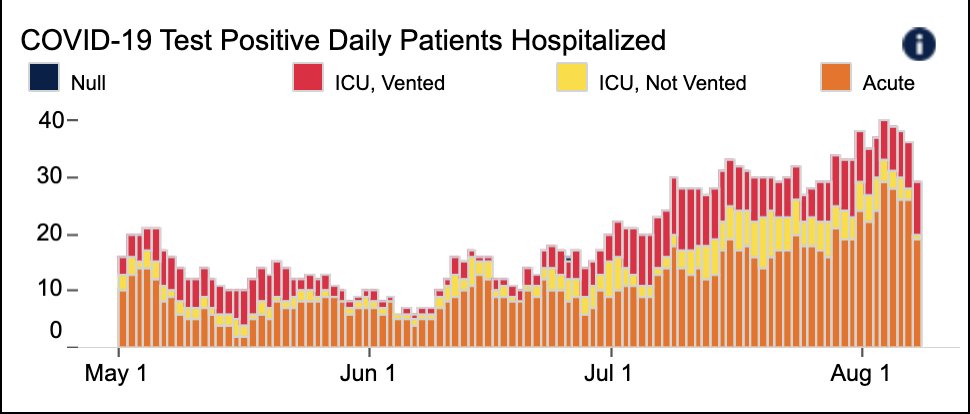
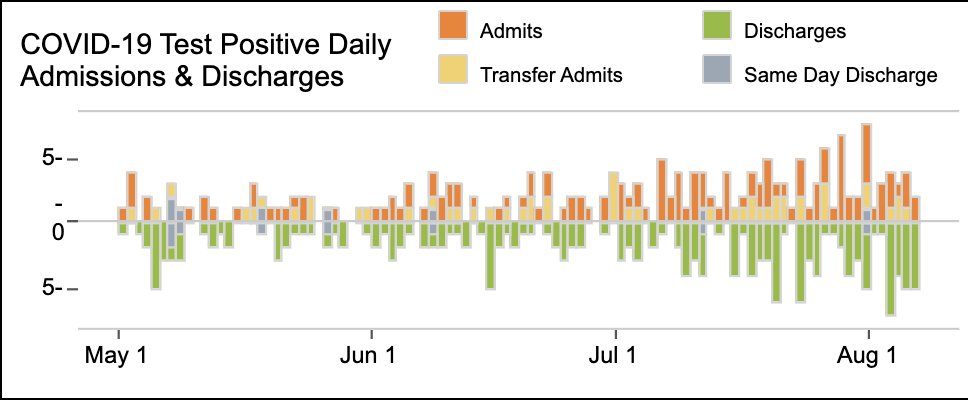
2/ First, local updates. Things are still OK @UCSF, SF, & CA. @UCSFHospitals, 29 pts, only 5 on vents (Fig) – lowest vent # in about a month. Interestingly, @ZSFGCare (our county hospital) has more Covid: 38 pts, 14 vents. In March/April, UCSF & ZSFG tended to run about even… 
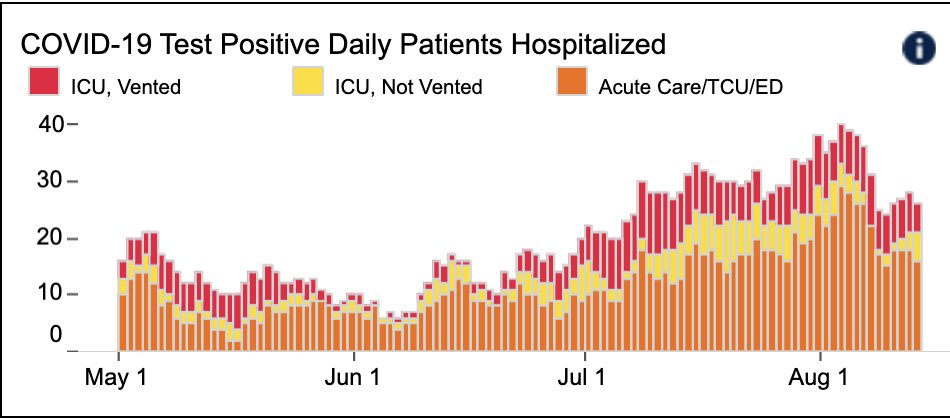
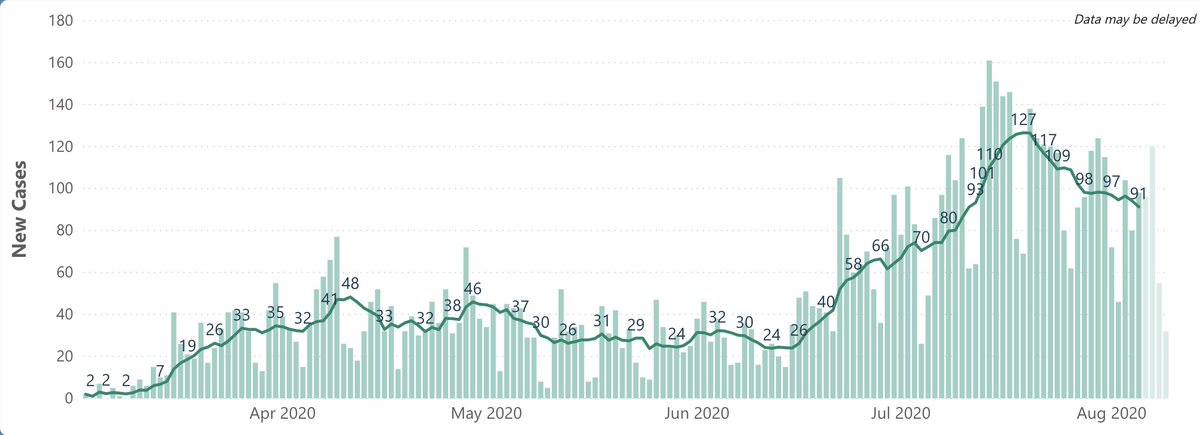
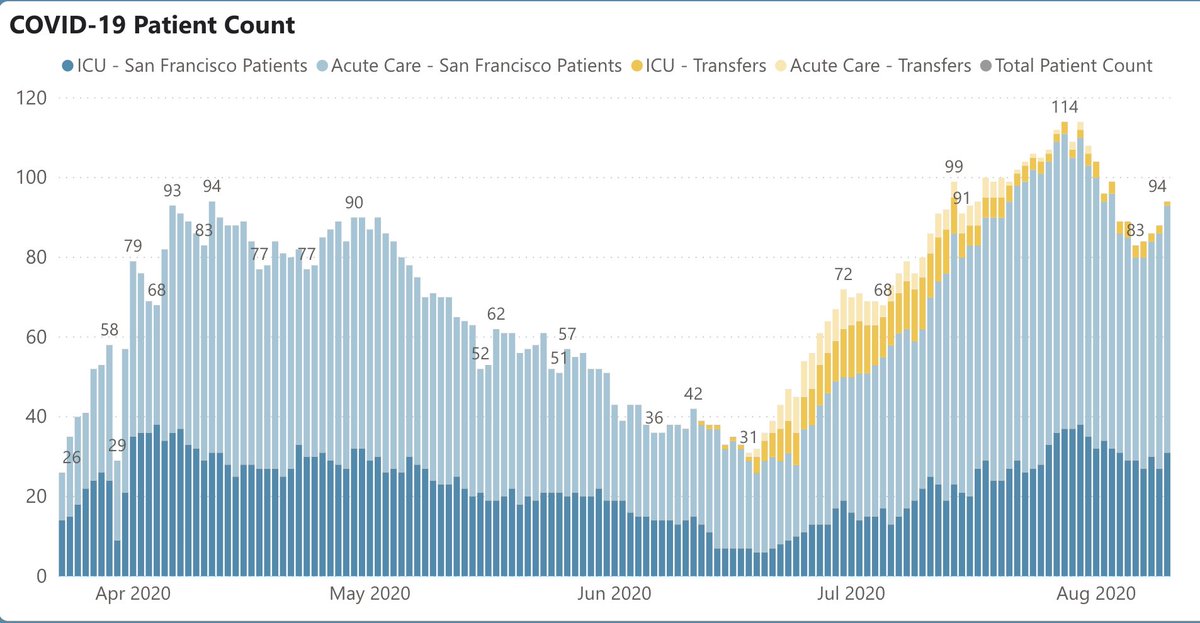
3/ …so this is likely another sign that Covid is hitting underserved populations more heavily, since ZSFG is city’s safety net hospital. SF is averaging 91 cases/d, down ~30% from peak last mth (Fig on L). Hospitalizations up a bit @ 94 (Fig R), but still well below peak of 114.
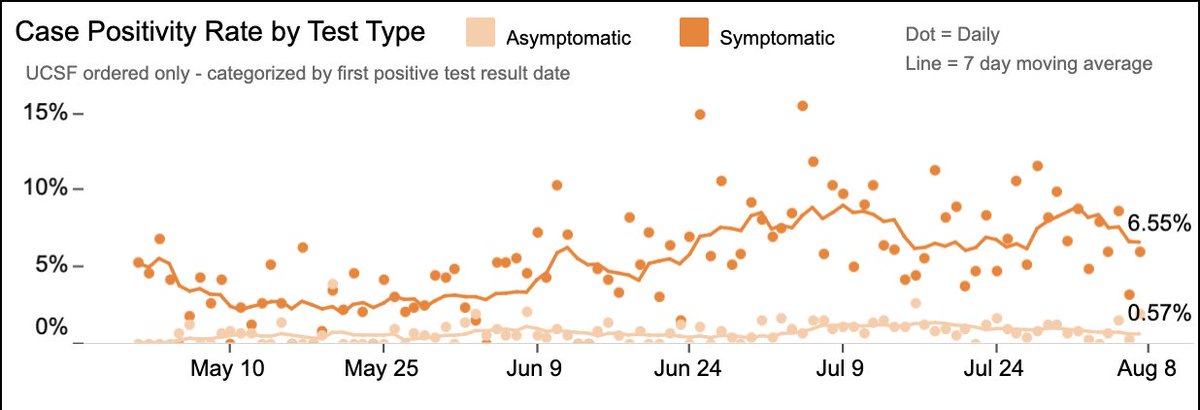
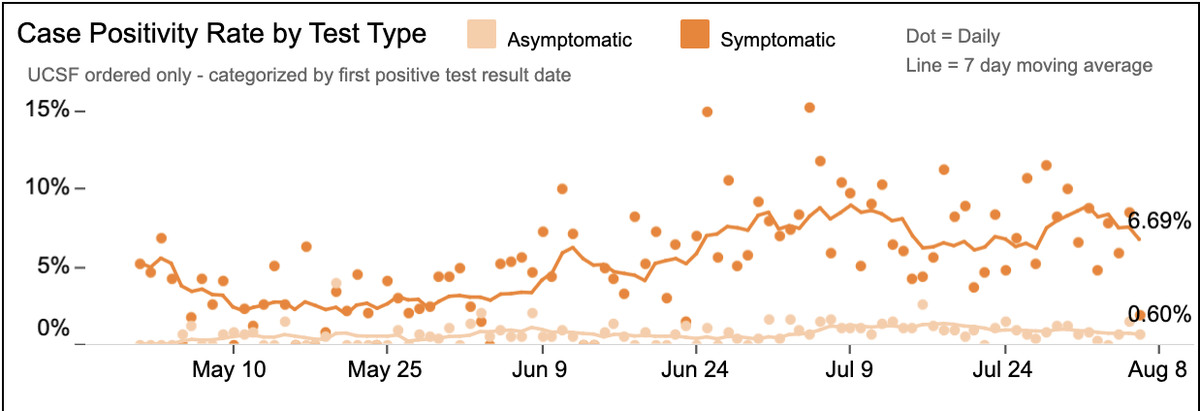
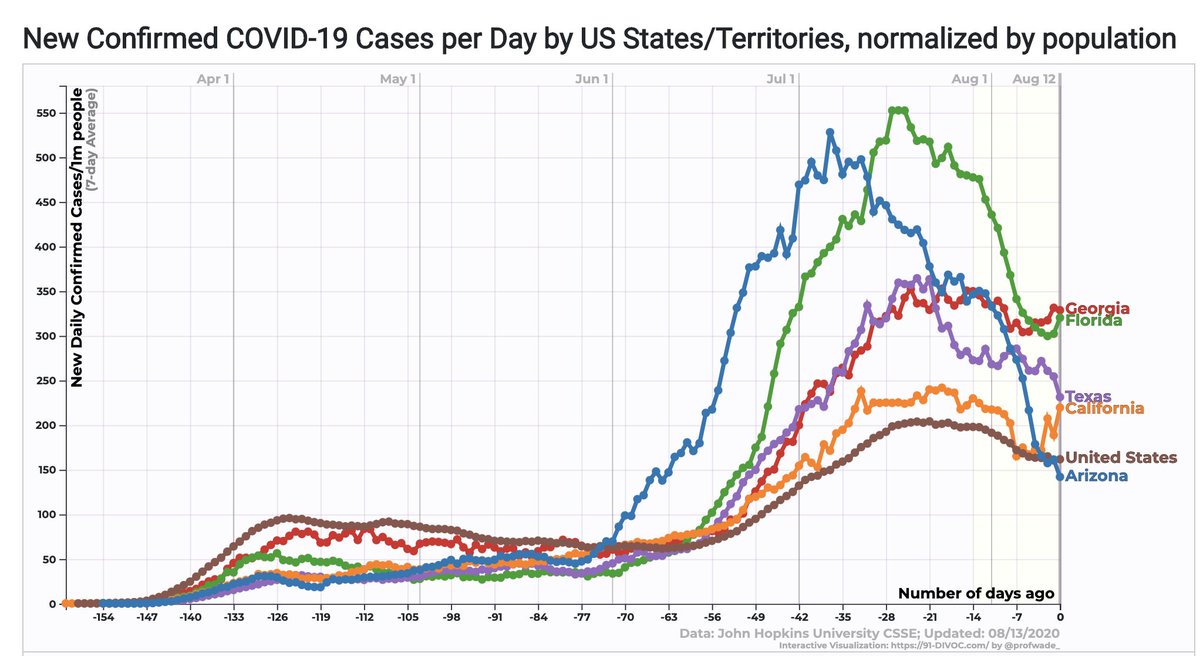
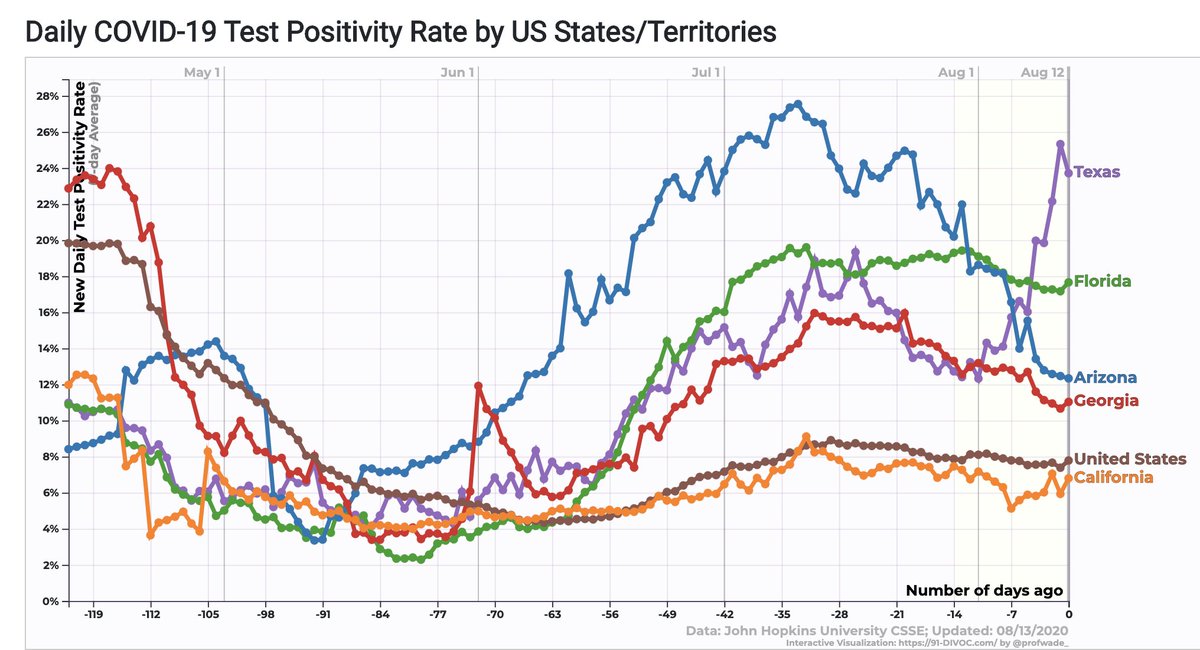
4/ CA numbers remain a bit suspect – mild uptick in case # ‘s; may be cases that were hiding in some lost database last wk. Overall CA is stable; not as sharp a downtrend as TX, FL, & AZ (Fig L). CA case positivity rate up a bit (now ~6.5%, Fig R); well below TX, Fl, AZ, & GA.
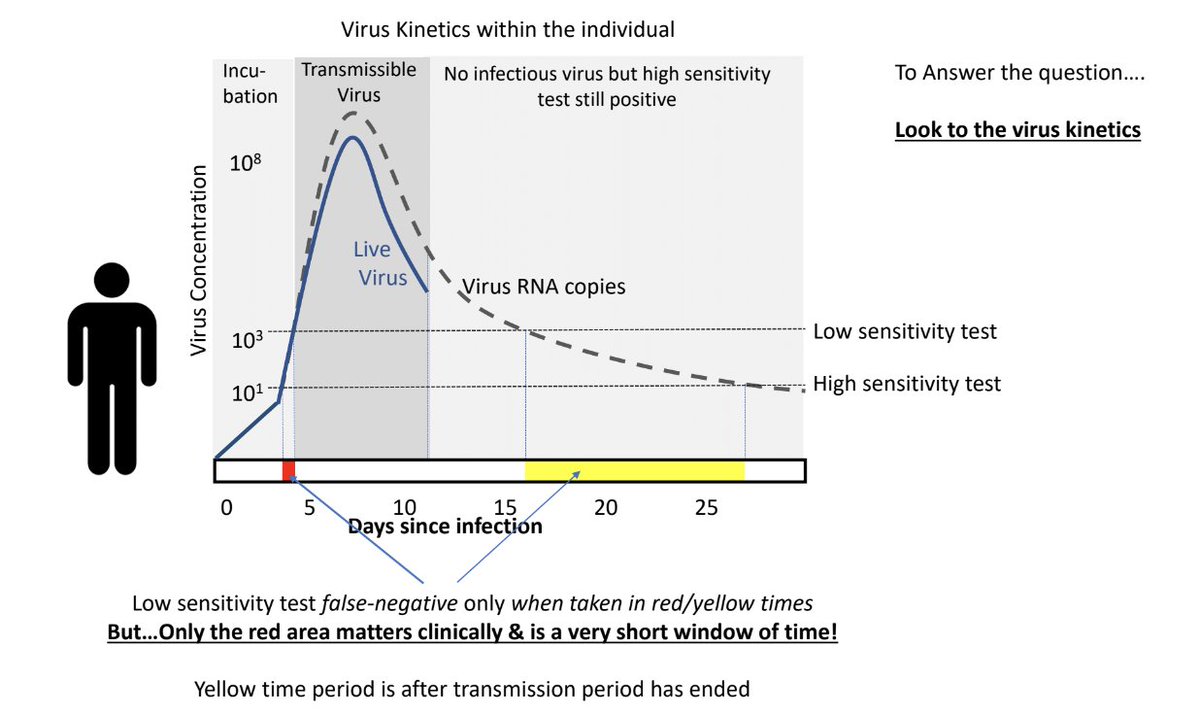
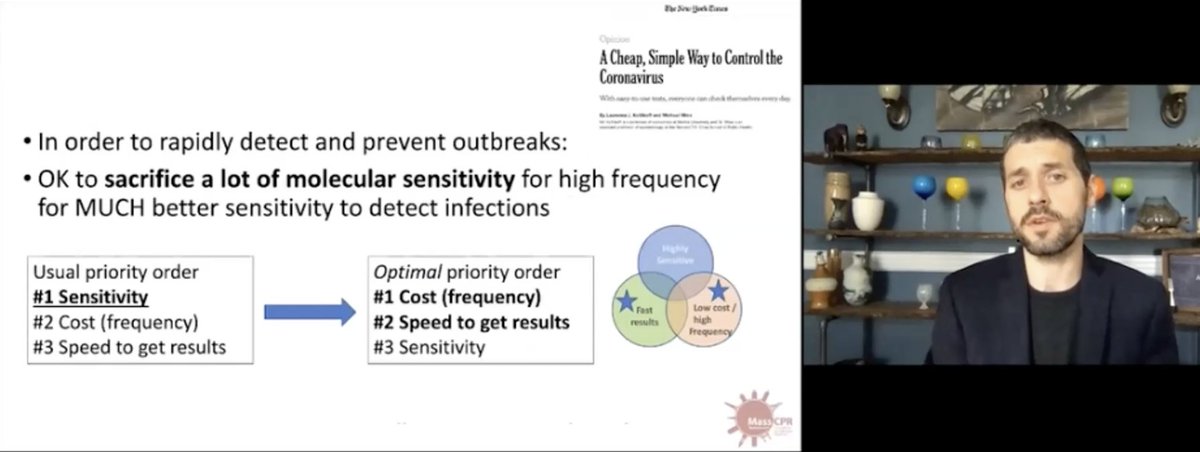
5/ On to grand rounds: 1st speaker: @michaelmina_lab @HarvardHSPH, who is studying a new paradigm for viral testing. He points out that usual PCR test for virus is more sensitive than it needs to be, finding many cases that have very low levels of virus, below transmission level.
6/ Unfortunately, PCR tests are expensive, not scalable, and pretty slow (thus testing delays). @ 9:50-19:30, Mina makes the case that trading off some sensitivity (in PCR) for cheap, highly accessible home antigen tests that can be used daily is optimal strategy for prevention.
7/ He's also making a more general point: we need to think about Covid testing differently – not as a medical diagnostic test (ie, does pt have Covid?) & more through a public health lens (can a cheap, scalable, good-enough test provide fast info that leads to safer behaviors?)
8/ So, while the MD thinks, “I need to know if this patient with a fever & cough has Covid, since, if she does, I’ll think differently about prognosis, whether to hospitalize, whether to start a Covid med like remdesivir or dexamethasone,” the public health professional thinks…
9/ ...“All I really care about is if this person is infectious. I don’t need to catch every last case of Covid; not a big deal if I miss one in a pt who isn’t capable of spread. I need fast, cheap, in-home or workplace tests that'll be + in folks who are shedding lots of virus.”
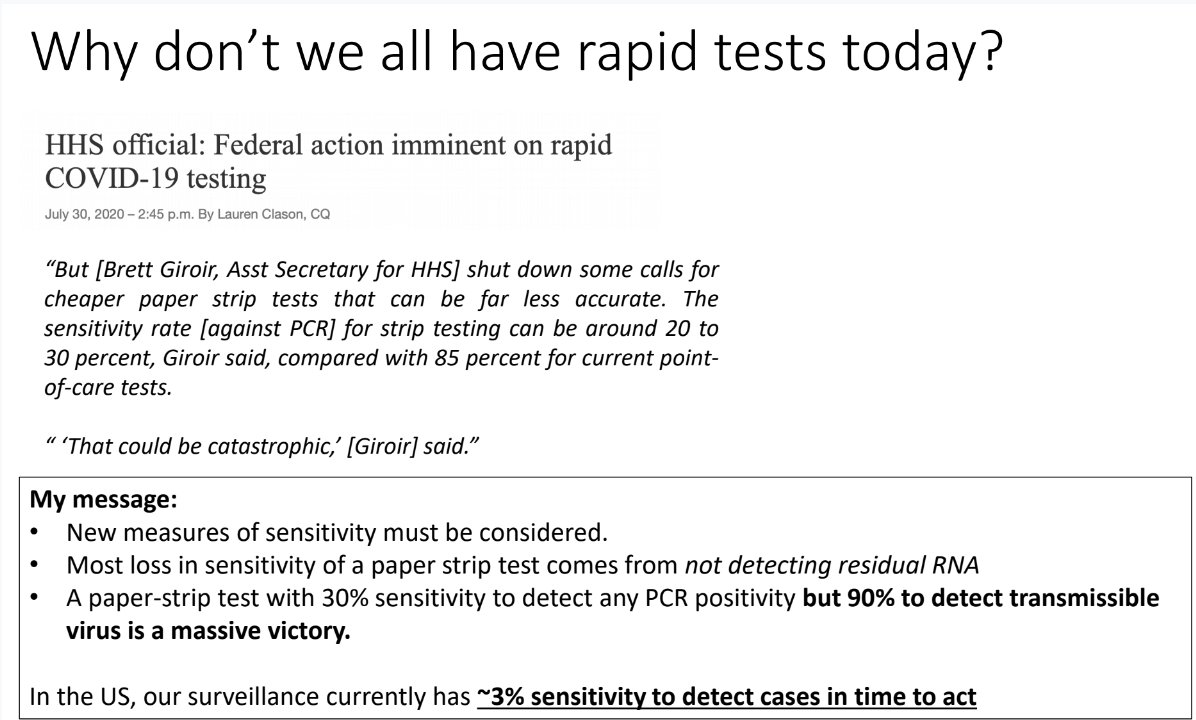
10/ @ 31:30, Mina describes nuts & bolts of rapid antigen tests: they're like pregnancy tests – put sample (saliva or swab from front of nose) onto test strip & look for color change. Estimated cost: ~$1/day. Goal: everybody tests at home every 1-3d, and quarantines if positive.
11/ Big obstacle: @US_FDA had no easy way to certify cheaper tests w/ lower sensitivity. Mina: “We don’t have a public health framework, we don’t have a regulatory pathway… to consider a test whose primary objective is one of public health and not individual health.”
12/ Clearly, Mina's plan can only work as part of a rethink of nat'l testing strategy & regulation. Unfortunately, chances this'll happen before November seem slim, since it would require big shift in FDA & some nat'l leadership. I hope it does; this paradigm makes tons of sense.
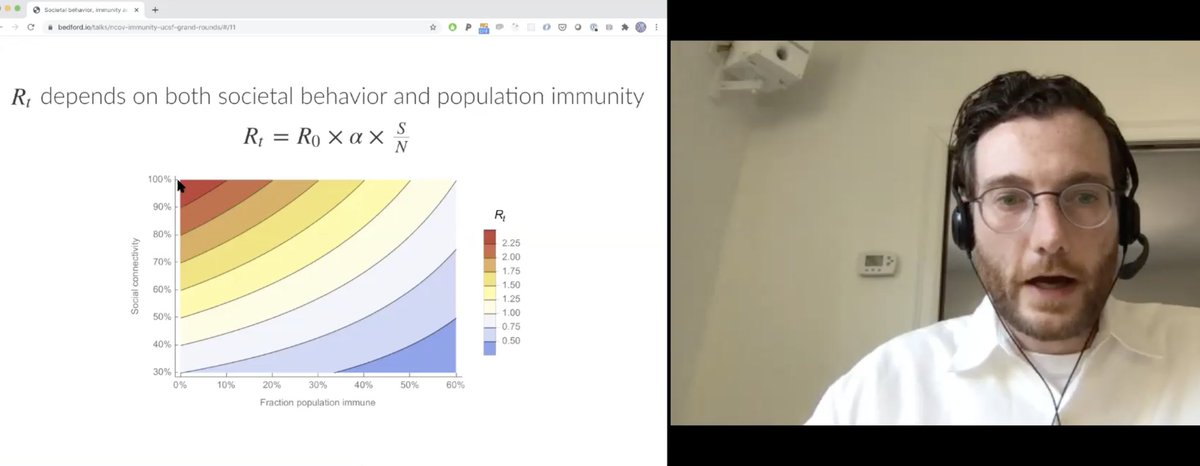
13/ Next up: Trevor Bedford @trvrb describes idea he raised on @Twitter tinyurl.com/y2zktlsq: that the classical herd immunity threshold of 60% may be too high, in that it doesn’t account for impact of behavioral change. @ 39:45-52:00, he elegantly reviews science & numbers.
14/ Figure shows that w/o behavioral change, need 60% of people immune to push transmission rate <1. But if you halve amount of “connectivity” (via masks, distancing), then you may reach equivalent of herd immunity at infection levels of ~20-30% (as in NYC, maybe FL?), not 60%
15/ I asked lots of questions (@ 52:40-1:05:30), incl.: whether behavioral change is dynamic (Answer: yes; “I can predict how virus is going to behave better than I can predict how people are going to behave”); Whether population modeling should reflect heterogeneous behavior…
16/ …ie, different segments of population engage in different risk-behaviors (Answer: yes, it would be more accurate); Does fact that San Quentin Covid hit rate is ~60% refute argument (Answer: no, probably no way to decrease "connectivity" at SQ because of conditions there)...
17/ … and, did his use of term “herd immunity” lead to some pushback, partisan or otherwise (Answer: yes, a lot – mostly that “you shouldn’t say that because it’ll cause people to behave less carefully.”)
But he feels that his job is to describe science clearly. Which he did.
But he feels that his job is to describe science clearly. Which he did.
18/ Today's final segment: @ESilvermanMD & @ash_mcmullenMD, both @ucsf, discuss the wonderful storytelling program @thenocturnists, & their two recent podcast series: “Stories From a Pandemic” & “Black Voices in Healthcare.”
19/ @ 1:06:25, Emily describes the origins of The Nocturnists (which she launched as a @ucsfmedicine resident): “I wanted to create a space to explore, to play, to tell stories about ourselves, & about our work… there was a lot of hunger for… creativity & communal catharsis.”
20/ @ 1:08:20, she describes her post-Covid strategy (which, of course, meant no live events): “We dropped everything…we were facing one of the biggest plot twists in medical history. We wanted to continue to be a space for self-expression, for healing, community & well-being.”
21/ “At 1:15:30, she plays a powerful 3 min clip of a Michigan MD describing her joy as (on her day off) she delivered convalescent plasma to a Covid pt in the ICU. Says Emily, accurately, “you’ll see how much she brings us into her world.” The artwork lends additional power.
22/ @ash_mcmullinMD, @ucsf faculty member based at our VA, describes her “Black Voices” series, launched after the George Floyd murder. In it, Ashley blends stories about healthcare/Covid and race. “I’m trying to elevate the humanity that can sometimes be absent in medicine.”
23/ @ 1:20:25, Ashley plays a beautiful clip (also ~3 min; w/ more great art) from a doctor who cares enough about her patient to braid the pt's matted hair. Ashley: “I hope the series allows a greater proximity to the Black experience through the lens of healthcare workers…”
25/ I'm back east, where it's hot. So, in a nod to authenticity, here's my full wardrobe for today’s Grand Rounds. I’m guessing I’m not the only one on Zoom dressed like this.
Hope you can watch whole GRs; here:
Stay safe, back tomorrow w/ weekly thread
Hope you can watch whole GRs; here:
Stay safe, back tomorrow w/ weekly thread