
1/ 45F p/w months of jaw swelling. Initially 1 nontender nodule, briefly improved after course of abxs-but she has been using makeup bc appeared bluish.
Now jaw feels "lumpy", one area draining, +trismus
Which would help define your suspect dx?
#IDTwitter #IDMedEd @ID_fellows
Now jaw feels "lumpy", one area draining, +trismus
Which would help define your suspect dx?
#IDTwitter #IDMedEd @ID_fellows
2/
Cervicofacial swelling (esp jaw) might bring ddx: cancer, TB, NTM, nocardia, and actinomyces.🔵color, brief abx response, sinus tract were clues for Actinomycosis!
Sulfur granules=classic but can be mis-ID'd as nocardia!
Tip:Nocardia+mycobact = acid fast, but actino are not
Cervicofacial swelling (esp jaw) might bring ddx: cancer, TB, NTM, nocardia, and actinomyces.🔵color, brief abx response, sinus tract were clues for Actinomycosis!
Sulfur granules=classic but can be mis-ID'd as nocardia!
Tip:Nocardia+mycobact = acid fast, but actino are not
3/
Actinomycosis
🔹Branching anaerobic GP
🔹Most common A.israelii but >40 spp
🔹Often polymicrobial inf: Aggregatibacter, Eikenella coordens, Fusobacterium, and more
🔹Nl flora: oral, GI, pulm, female GU tracts
🔹As always, great pics via @richdavisphd !
Actinomycosis
🔹Branching anaerobic GP
🔹Most common A.israelii but >40 spp
🔹Often polymicrobial inf: Aggregatibacter, Eikenella coordens, Fusobacterium, and more
🔹Nl flora: oral, GI, pulm, female GU tracts
🔹As always, great pics via @richdavisphd !
4/
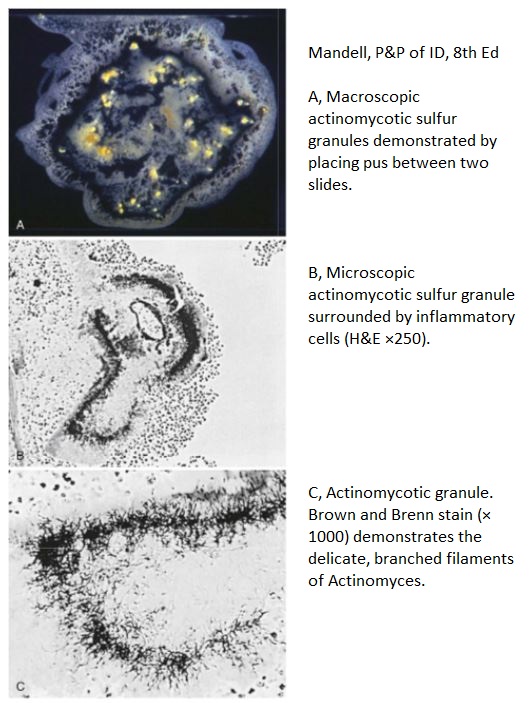
🔸Special media not required, but semiselective media may ⬆️isolation
🔸A.israelii “molar tooth” colony
🔸Characteristic sulfur granules in vivo. Misnomer🚨, theres no sulfur! just appears yellow in pus. actually = tangle of 🦠➡️round basophilic masses with terminal "clubs"
🔸Special media not required, but semiselective media may ⬆️isolation
🔸A.israelii “molar tooth” colony
🔸Characteristic sulfur granules in vivo. Misnomer🚨, theres no sulfur! just appears yellow in pus. actually = tangle of 🦠➡️round basophilic masses with terminal "clubs"

5/
Pathogenesis often relies on disruption of mucosal barrier, examples:
🔹Oral/cervicofacial: dental/oral surg, trauma, H&N radiotherapy or procedures
🔹Pulm: aspiration
🔹GI: Surgery, diverticulitis, appy, foreign bodies
May have component of biofilm (think IUD association)
Pathogenesis often relies on disruption of mucosal barrier, examples:
🔹Oral/cervicofacial: dental/oral surg, trauma, H&N radiotherapy or procedures
🔹Pulm: aspiration
🔹GI: Surgery, diverticulitis, appy, foreign bodies
May have component of biofilm (think IUD association)
6/
Classic actinomycosis features:
✳️Dense fibrotic lesions or masses ("wooden"), can be solid + mistaken for malignancy!
✳️Slow contiguous spread
✳️Ignores tissue planes!
✳️Sinus tracts (can heal and re-form)
✳️Red/blue hue to skin
✳️Refractory/relapsing after short abx course
Classic actinomycosis features:
✳️Dense fibrotic lesions or masses ("wooden"), can be solid + mistaken for malignancy!
✳️Slow contiguous spread
✳️Ignores tissue planes!
✳️Sinus tracts (can heal and re-form)
✳️Red/blue hue to skin
✳️Refractory/relapsing after short abx course
7/
Most recognized actinomycosis = oral-cervicofacial dz
🔹Classic = painless perimandibular mass
🔹May present as chronic recurrent abscess or appear solid like malignancy
🔹Can extend contiguously to structures (carotid, orbits, spine, etc). Trismus is affects mastic muscles
Most recognized actinomycosis = oral-cervicofacial dz
🔹Classic = painless perimandibular mass
🔹May present as chronic recurrent abscess or appear solid like malignancy
🔹Can extend contiguously to structures (carotid, orbits, spine, etc). Trismus is affects mastic muscles
8/
Key clinical settings for cervicofacial dz:
🔸Dental caries/extractions, gingival trauma
🔸DM, immunosuppression
🔸Infected osteoradionecrosis as complication after H&N radiation therapy
🔸Bisphosphonate-associated osteonecrosis
pubmed.ncbi.nlm.nih.gov/19886792/
Key clinical settings for cervicofacial dz:
🔸Dental caries/extractions, gingival trauma
🔸DM, immunosuppression
🔸Infected osteoradionecrosis as complication after H&N radiation therapy
🔸Bisphosphonate-associated osteonecrosis
pubmed.ncbi.nlm.nih.gov/19886792/
9/
Other big ones:
✳️Thoracic dz: can be aspiration vs direct extension
▪️No classic radiographic feature but keys that may indicate actino: contiguous bony/rib dz, involvement of mediastinal, pleural thickening or empyema
✳️Abdominal dz: more in next tweet
Other big ones:
✳️Thoracic dz: can be aspiration vs direct extension
▪️No classic radiographic feature but keys that may indicate actino: contiguous bony/rib dz, involvement of mediastinal, pleural thickening or empyema
✳️Abdominal dz: more in next tweet
10/
▪️Can present as abscess vs firm mass. Sinus tracts may come late
▪️R iliac fossa is freq site + appendicitis is common predisposing event
✳️Pelvic dz: finding actino on pap smear with IUD place can be incidental ➡️ but s/s PID should prompt IUD removal, cxs, pelvic US
▪️Can present as abscess vs firm mass. Sinus tracts may come late
▪️R iliac fossa is freq site + appendicitis is common predisposing event
✳️Pelvic dz: finding actino on pap smear with IUD place can be incidental ➡️ but s/s PID should prompt IUD removal, cxs, pelvic US
11/
💊Tx: high dose PCN
💊Alternatives CTX, amox, doxy, macrolides
💊Remember that might need to treat copathogens (eg reaching for amox-clav instead)
💊Optimal duration depends on burden of disease and location - can be prolonged (months)
💊Tx: high dose PCN
💊Alternatives CTX, amox, doxy, macrolides
💊Remember that might need to treat copathogens (eg reaching for amox-clav instead)
💊Optimal duration depends on burden of disease and location - can be prolonged (months)
12/
Actinomycosis is uncommon but known for being great mimicker! often mistaken as malignancy, TB, nocardia, endemic fungal dz. Remember to consider this is has the right clinical features.
Here is two reviews you can check out: pubmed.ncbi.nlm.nih.gov/21990282/
pubmed.ncbi.nlm.nih.gov/25045274/
Actinomycosis is uncommon but known for being great mimicker! often mistaken as malignancy, TB, nocardia, endemic fungal dz. Remember to consider this is has the right clinical features.
Here is two reviews you can check out: pubmed.ncbi.nlm.nih.gov/21990282/
pubmed.ncbi.nlm.nih.gov/25045274/


