1/ #CNCR continues with another @cardionerds case from @UTSWCardfellow
Catch up on the episode here: cardionerds.com/47-syphilitic-…
Here’s a brief re-cap with some of the 💯 learning.
First a synopsis…
Catch up on the episode here: cardionerds.com/47-syphilitic-…
Here’s a brief re-cap with some of the 💯 learning.
First a synopsis…
2/ ...Man in his 50s p/w 3m of ⬆️DOE, orthopnea, and LE edema that suddenly worsened in the last 2d.
No other hx. Prefers male partners.
P/w wide pulse pressure and exam concerning for severe AR.
What's your approach to causes of AR?
No other hx. Prefers male partners.
P/w wide pulse pressure and exam concerning for severe AR.
What's your approach to causes of AR?
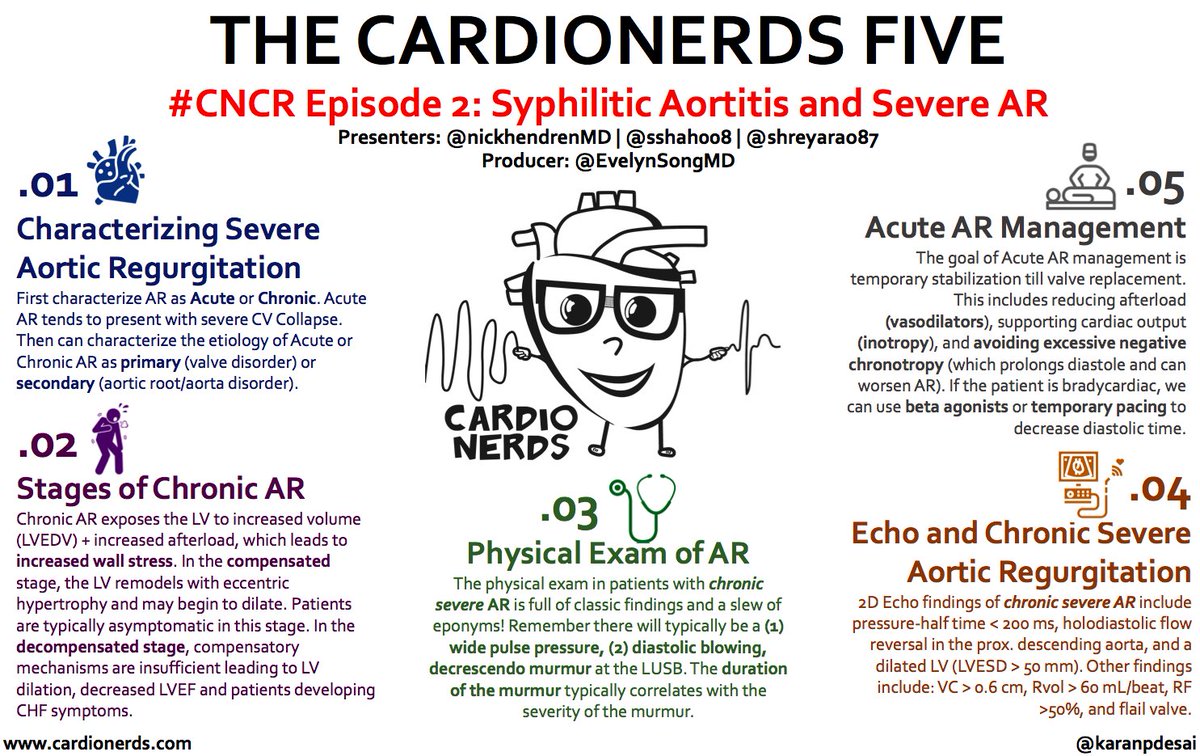
3/ First think of AR as Acute or Chronic!
Acute severe AR tends to present w/ hypotension + ❤️shock
➡️...then can think of as a primary valve issue or secondary due to aortic root/aortic disease.
Acute severe AR tends to present w/ hypotension + ❤️shock
➡️...then can think of as a primary valve issue or secondary due to aortic root/aortic disease.

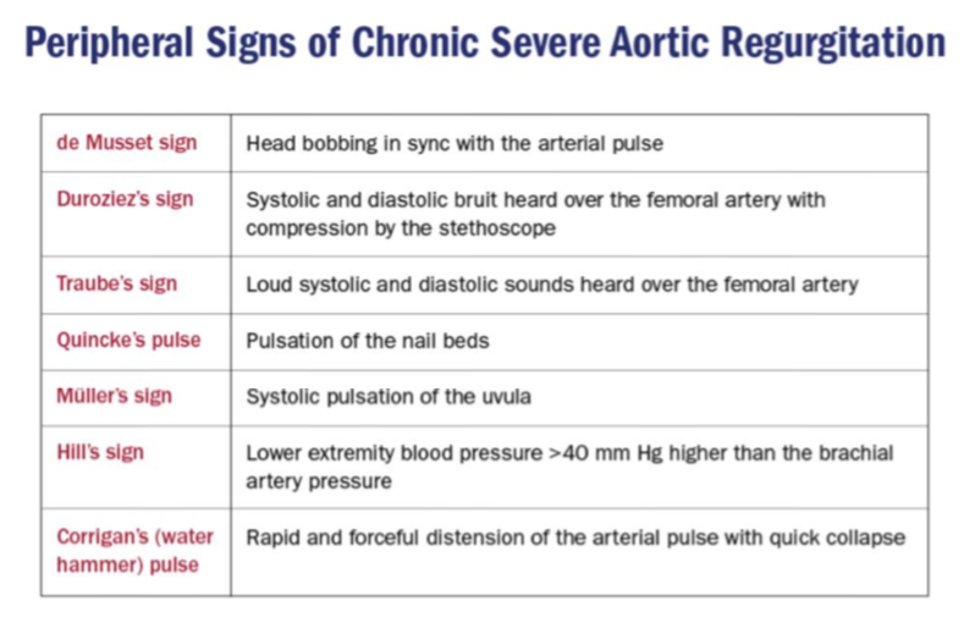
4/ What are the physical exam findings of chronic AR?
There are many eponyms associated with AR. See below! These findings in general are related to the wide pulse pressure
Classic AR murmur = diastolic, blowing, decrescendo murmur at the left sternal border
There are many eponyms associated with AR. See below! These findings in general are related to the wide pulse pressure
Classic AR murmur = diastolic, blowing, decrescendo murmur at the left sternal border
5/ What correlates with AR severity on exam?
6/ Duration > Intensity ~ with severity of AR.
Early on --> the AR murmur is typically short and then becomes pan-diastolic.
‼️ - remember though the murmur may shorten again in later AR because Aortic and LV pressures may rapidly equilibrate
Back to the case...
Early on --> the AR murmur is typically short and then becomes pan-diastolic.
‼️ - remember though the murmur may shorten again in later AR because Aortic and LV pressures may rapidly equilibrate
Back to the case...
7/ TTE showed holodiastolic flow reversal in the thoracic aorta and RHCx showed equalization of LVEDP (black) and aortic diastolic pressure (red) at 40mmHg with a CO of 1.73
What's the mechanism behind holodiastolic flow reversal?
What's the mechanism behind holodiastolic flow reversal?

8/ The holodiastolic flow reversal = retrograde flow back in to LV during diastole
Some flow reversal is normal in early diastole (coronary perfusion!) – but high velocity and throughout diastole is abnormal
If you see it in the Abdominal Aorta – severe AR is likely!
Some flow reversal is normal in early diastole (coronary perfusion!) – but high velocity and throughout diastole is abnormal
If you see it in the Abdominal Aorta – severe AR is likely!

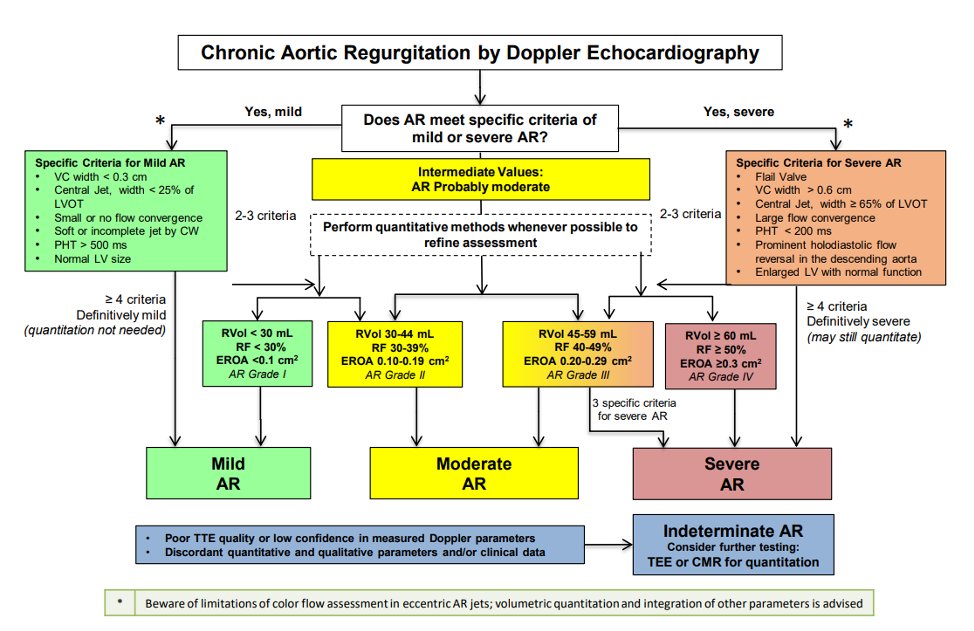
9/ Don't be fooled!
When assessing AR severity, use a multi-parametric approach, considering multiple variables. See 2D echo parameters below
When assessing AR severity, use a multi-parametric approach, considering multiple variables. See 2D echo parameters below
10/ Now... our pt is in ❤️ shock 2/2 acute AR.
‼️... acute AR is a hemodynamic emergency! Goal = surgery
Pearls:
⬇️HR = ⬆️⏰in diastole = ⬆️ AR
⬆️HR = ⬇️⏰in diastole = ⬇️ AR
🚫neg chronotropic agents
If pt is brady, may use maneuvers to ⬆️HR like B-agonist & temp. pacing
‼️... acute AR is a hemodynamic emergency! Goal = surgery
Pearls:
⬇️HR = ⬆️⏰in diastole = ⬆️ AR
⬆️HR = ⬇️⏰in diastole = ⬇️ AR
🚫neg chronotropic agents
If pt is brady, may use maneuvers to ⬆️HR like B-agonist & temp. pacing
11/ What are the indications for AVR in AR?
Class I indications for AVR in AR:
> Symptomatic severe AR regardless of EF
> Asymptomatic severe AR WITH LVEF <50% 2/2 AR
> Severe AR and undergoing cardiac surgery for other indications
Class I indications for AVR in AR:
> Symptomatic severe AR regardless of EF
> Asymptomatic severe AR WITH LVEF <50% 2/2 AR
> Severe AR and undergoing cardiac surgery for other indications

12/ Want to know the rest of the case? Listen to the full discussion and more notes on the blog!
cardionerds.com/47-syphilitic-…
Thanks again to @nickhendrenMD @shreyarao87 @sshah008 for sharing this case, to @cardionerds for this opportunity, and to @karanpdesai for his mentorship!
cardionerds.com/47-syphilitic-…
Thanks again to @nickhendrenMD @shreyarao87 @sshah008 for sharing this case, to @cardionerds for this opportunity, and to @karanpdesai for his mentorship!
• • •
Missing some Tweet in this thread? You can try to
force a refresh