
1/ Here are the relative effects (Y axis) and the p-values (X axis) found for all the 6 clinical outcomes measured by the 3 outpatient RCTs of HCQ for covid (Boulware, Skipper, Mitjà).
Positive Y is benefit, negative Y is harm
See a pattern?
Positive Y is benefit, negative Y is harm
See a pattern?
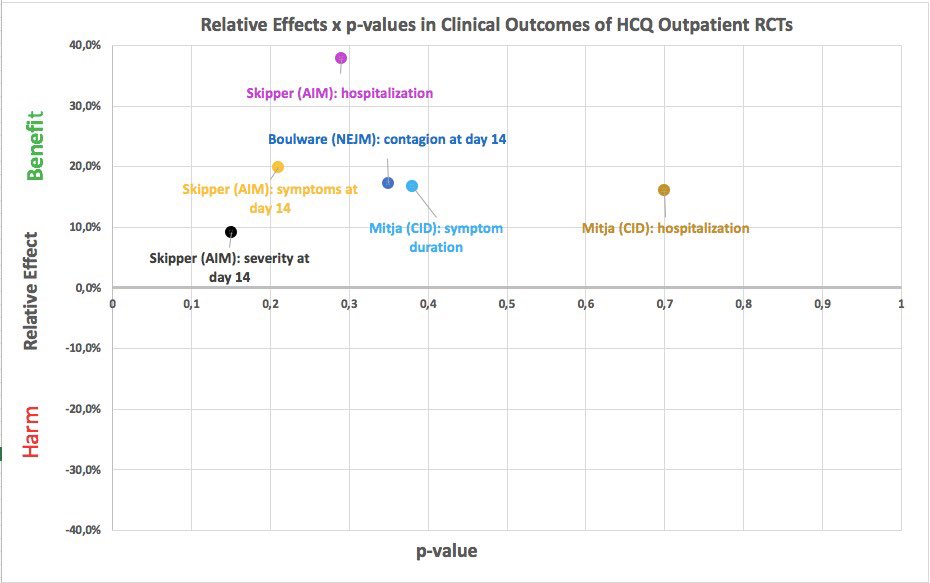
2/ To spell it out: the treatment groups did better than the control groups, with p-values > 0,05, in all 6 clinical outcomes -- hospitalization, duration and severity of symptoms -- in the 3 published RCTs of HCQ for outpatients (Boulware NEJM, Skipper AIM, Mitjà CID)
3/ This suggests that these RCTs are measuring real effects but are underpowered. Very unlikely to be a due to coincidence, especially after one digs into the details of the data.
4/ Group sizes range from about 150 (in Mitjà) to about 400 (in Boulware)
This is underpowered for relative effects of ~20% in bad outcomes that are rare in baseline, especially for the young (~40yrs old median) cohorts in these RCTs
This is underpowered for relative effects of ~20% in bad outcomes that are rare in baseline, especially for the young (~40yrs old median) cohorts in these RCTs
5/ Youth dilutes the effect, if real (as most likely it is).
So does treatment delay:
* randomization 1 to 4 days after symptom onset in Boulware+Skipper, plus shipping delay
* treatment (or randomization?) median of 4 days after symptom onset in Mitjà
So does treatment delay:
* randomization 1 to 4 days after symptom onset in Boulware+Skipper, plus shipping delay
* treatment (or randomization?) median of 4 days after symptom onset in Mitjà
6/ The three RCTs are HCQ-only and suggest relative effects of ~20%. Probably larger if taken say on day 2 or 3 after treatment onset.
(Various groups have been looking into this, including from "prestigious" international universities -- prestige shouldn't matter, but does.)
(Various groups have been looking into this, including from "prestigious" international universities -- prestige shouldn't matter, but does.)
7/ In practice, early outpatients have mostly used the HCQ+azithromycin combination
The observational studies suggest that the effect of HCQ+azithromycin is larger than that of HCQ alone -- but still not a miracle cure. Maybe ~50% reduction on hospitalization.
The observational studies suggest that the effect of HCQ+azithromycin is larger than that of HCQ alone -- but still not a miracle cure. Maybe ~50% reduction on hospitalization.
8/ No antiviral effect in Mitjà (and some others). So that may not be the underlying mechanism.
But the empirical evidence on clinical outcomes says the effect (almost certainly) is real. Action is immunomodulatory? Other(s)? Time to dig deeper, not fight the data.
But the empirical evidence on clinical outcomes says the effect (almost certainly) is real. Action is immunomodulatory? Other(s)? Time to dig deeper, not fight the data.
9/ I'd plot the incidence of Torsades de Pointes in the HCQ outpatient studies, but there is nothing to plot: there were none. Neither in the RCTs nor in the observational ones. Zero cases.
So it's safe. Which comes as a shocking revelation to 0% of the world's rheumathologists
So it's safe. Which comes as a shocking revelation to 0% of the world's rheumathologists
10/ In sum, early treatment with HCQ for outpatients:
* safe (except if patient has specific contraindication for HCQ)
* almost certainly has effect, about ~20% reduction in main bad outcomes
* effect may be stronger for early treatment with HCQ+azithromycin
* safe (except if patient has specific contraindication for HCQ)
* almost certainly has effect, about ~20% reduction in main bad outcomes
* effect may be stronger for early treatment with HCQ+azithromycin
11/ So many doctors and medical researchers incurring in the p < 0.05 "bright line" fallacy. It's depressing.
The American Statistical Association has pointed out this basic trap years ago but researchers keep falling into it:
statsmadeeasy.net/2016/08/bright…
The American Statistical Association has pointed out this basic trap years ago but researchers keep falling into it:
statsmadeeasy.net/2016/08/bright…
12/ This subject has been absurdly politicized. People have been the target of substantial online aggression for touching it. The aggression has come both from the "HCQ is a miracle cure" and the "outpatient HCQ is dangerous and proven to be ineffective" crowds.
13/ Some symptoms of the madness around the subject:
13.i. "I loathe politician X, so if X says HCQ works then HCQ cannot work"
13.ii. "I adore politician X, so if X says HCQ works then X must work"
13.i. "I loathe politician X, so if X says HCQ works then HCQ cannot work"
13.ii. "I adore politician X, so if X says HCQ works then X must work"
13/ Some symptoms of the madness around the subject:
13.iii. "The Society of such-and-such has said it doesn't work, so it doesn't"
(one society insisted until June that masks should be used by health workers only, another that offices should stay open in Brazil in mid-March)
13.iii. "The Society of such-and-such has said it doesn't work, so it doesn't"
(one society insisted until June that masks should be used by health workers only, another that offices should stay open in Brazil in mid-March)
13/ Some symptoms of the madness around the subject:
13.iv. "Such-and-such prestigious journal has proved it does not work"
(this one was very common in the days following publication of the Surgisphere fraud in the Lancet)
13.iv. "Such-and-such prestigious journal has proved it does not work"
(this one was very common in the days following publication of the Surgisphere fraud in the Lancet)
13/ Some symptoms of the madness around the subject:
13.v. "Only experts must be heard"
Foolish in the first place. Double foolish when targeted at groups that include mathematicians, biostatisticians, and medical researchers
13.v. "Only experts must be heard"
Foolish in the first place. Double foolish when targeted at groups that include mathematicians, biostatisticians, and medical researchers
13/ Some symptoms of the madness around the subject:
13.vi. "If a treatment doesn't work in more advanced stage, then it shouldn't work in early stage"
Heard this one from a medical researcher. Yes, really.
13.vi. "If a treatment doesn't work in more advanced stage, then it shouldn't work in early stage"
Heard this one from a medical researcher. Yes, really.
13/ Some symptoms of the madness around the subject:
13.vii. "Covid is just a benign flu and if you take HCQ then you're 100% safe from it"
This one manages to contradict both the data and itself
13.vii. "Covid is just a benign flu and if you take HCQ then you're 100% safe from it"
This one manages to contradict both the data and itself
13/ Some symptoms of the madness around the subject:
13.viii. "Treatments should only be used after RCTs with p<0.05"
If followed, this bright-line thinking would immediately halt the use of blood thinners, plasma, and proning by hospitals
13.viii. "Treatments should only be used after RCTs with p<0.05"
If followed, this bright-line thinking would immediately halt the use of blood thinners, plasma, and proning by hospitals
13/ Some symptoms of the madness around this subject:
13.ix. "If this plot is any good, why isn't it published in a peer-reviewed journal?"
Getting some of that too. When reality beats satire...
13.ix. "If this plot is any good, why isn't it published in a peer-reviewed journal?"
Getting some of that too. When reality beats satire...

